

Assessing the prevalence and impact of preserved ratio impaired spirometry in low-income and middle-income countries: a post-hoc cross-sectional analysis
- PMID: 39151984
- PMCID: PMC12404211
- DOI: 10.1016/S2214-109X(24)00233-X
Assessing the prevalence and impact of preserved ratio impaired spirometry in low-income and middle-income countries: a post-hoc cross-sectional analysis
Abstract
Background: More than 90% of the morbidity and mortality from chronic respiratory disease occurs in low-income and middle-income countries (LMICs), with substantial economic impact. Preserved ratio impaired spirometry (PRISm) is a prevalent lung function abnormality associated with increased mortality in high-income countries. We aimed to conduct a post-hoc analysis of a cross-sectional study to assess the prevalence of, the risk factors for, and the impact of PRISm in three diverse LMIC settings.
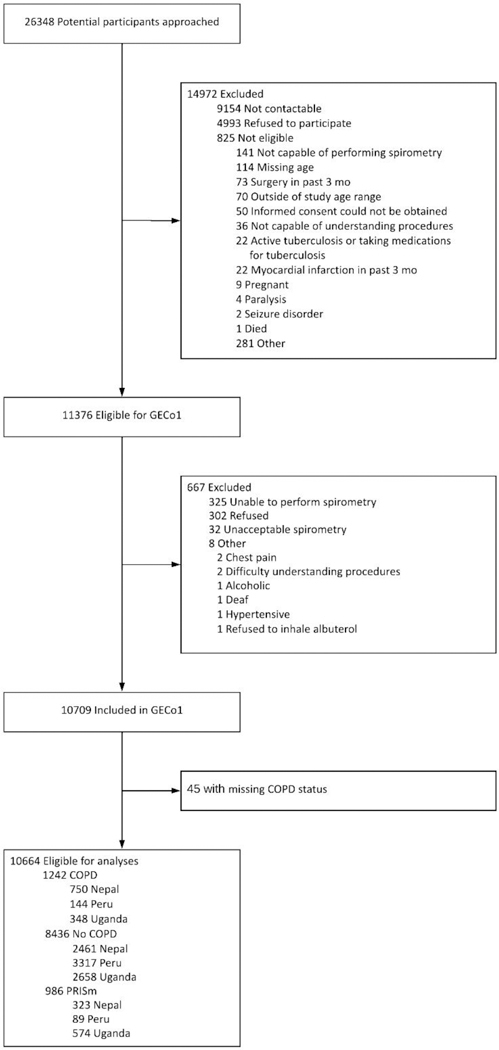
Methods: We recruited a random, age-stratified and sex-stratified sample of the population in semi-urban Bhaktapur, Nepal; urban Lima, Peru; and rural Nakaseke, Uganda. Quality-assured post-bronchodilator spirometry was performed to American Thoracic Society standards and PRISm was defined as a forced expiratory volume in one second (FEV1) of less than 80% predicted with a FEV1/forced vital capacity ratio of 0·70 or more. We used t tests and χ2 analyses to assess the relationships between demographic, biometric, and comorbidity variables with PRISm. Multivariable logistic models with random intercept by site were used to estimate odds ratios (ORs) with 95% CIs.
Findings: 10 664 participants were included in the analysis, with a mean (SD) age of 56·3 (11·7) years and an equal distribution by sex. The prevalence of PRISm was 2·5% in Peru, 9·1% in Nepal, and 16·0% in Uganda. In multivariable analysis, younger age (OR for each decile of age 0·87, 95% CI 0·82-0·92) and being female (1·37, 1·18-1·58) were associated with increased odds of having PRISm. Biomass exposure was not consistently associated with PRISm across sites. Individuals with PRISm had impairment in respiratory-related quality of life as measured by the St George's Respiratory Questionnaire (OR by decile 1·18, 95% CI 1·10-1·25).
Interpretation: The prevalence of PRISm is heterogeneous across LMIC settings and associated with age, female sex, and biomass exposure, a common exposure in LMICs. A diagnosis of PRISm was associated with worse health status when compared with those with normal lung function. Health systems in LMICs should focus on all spirometric abnormalities as opposed to obstruction alone, given the disease burden, reduced quality of life, and size of the undiagnosed population at risk.
Funding: Medical Research Council.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests TS reports grants or contracts from the Australian Lung Health Initiative; consulting fees from Verona Pharmaceuticals; and a leadership or fiduciary role in board, society, committee, or advocacy groups for 4D Medical. OF-F reports a Global Emerging Leader Award grant from the Fogarty International Centre. JJM reports grant support and payments made to their institution from the Alliance for Health Policy and Systems Research, Bloomberg Philanthropies, FONDECYT via CIENCIACTIVA and CONCYTEC, the British Council, British Embassy, the Newton-Paulet Fund, the UK Department for International Development, the UK Medical Research Council, the Wellcome Global Health Trials partnership, the Fogarty International Center, Grand Challenges Canada, the International Development Research Center Canada, Inter-American Institute for Global Change Research, the National Cancer Institute, National Heart, Lung, and Blood Institute, National Institute of Mental Health, the Swiss National Science Foundation, the UK Research and Innovation (UKRI) Biotechnology and Biological Sciences Research Council, the UKRI Engineering and Physical Sciences Research Council, the UKRI Medical Research Council, the Wellcome Trust, and the World Diabetes Foundation; a contract from Health Action International; consulting fees from the Pan American Health Organization and Bloomberg Philanthropies; participation on data safety monitoring or advisory boards for the Nigeria Sodium Study, the Intensive care bundle with blood pressure Reduction in Acute Cerebral haemorrhage Trial, the Latin American Brain Health institute, Universidad Adolfo Ibáñez (Chile), Programa de Gastronomía, Facultad de Estudios Interdisciplinarios, Pontificia Universidad Católica del Perú, and the InterAmerican Heart Foundation; being Co-chair of the Independent Group of Scientists, 2023 Global Sustainable Development Report, UN; being a member of the Scientific Expert Committee, Global Data Collaborative for CV Population Health, the World Health Federation, Microsoft, and Novartis Foundation; being a member of the Scientific and Technical Advisory Committee for the Alliance for Health Policy and Systems Research, WHO; being a member of WHO's Technical Advisory Group on non-communicable disease-related research and innovation, Non-communicable Diseases Department, WHO; and being a member of the Advisory Scientific Committee, Instituto de Investigación Nutricional, Peru. All other authors declare no competing interests.
Figures

References
-
- Burney P, Jarvis D, Perez-Padilla R. The global burden of chronic respiratory disease in adults. The International Journal of Tuberculosis and Lung Disease 2015; 19(1): 10–20. - PubMed
-
- Buist AS, McBurnie MA, Vollmer WM, et al. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. The Lancet 2007; 370(9589): 741–50. - PubMed
-
- Menezes AMB, Perez-Padilla R, Jardim JB, et al. Chronic obstructive pulmonary disease in five Latin American cities (the PLATINO study): a prevalence study. The Lancet 2005; 366(9500): 1875–81. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
