

A retrospective study of prognostic factors and prostate-specific antigen dynamics in Japanese patients with metastatic hormone-sensitive prostate cancer who received combined androgen blockade therapy with bicalutamide
- PMID: 39153094
- PMCID: PMC11420257
- DOI: 10.1007/s10147-024-02597-x
A retrospective study of prognostic factors and prostate-specific antigen dynamics in Japanese patients with metastatic hormone-sensitive prostate cancer who received combined androgen blockade therapy with bicalutamide
Abstract
Background: This retrospective observational study explored the therapeutic potential of combined androgen blockade (CAB) with bicalutamide (Bic-CAB) as an initial treatment for metastatic hormone-sensitive prostate cancer (mHSPC) in Japan.
Methods: The electronic health records of 159 patients with mHSPC from three Japanese institutions who received initial treatment with Bic-CAB between 2007 and 2017 were analyzed. The time to prostate-specific antigen (PSA) progression, duration of Bic-CAB treatment, and overall survival (OS), with various definitions for PSA progression, were assessed. A multivariate Cox proportional hazards model was constructed using clinical parameters to predict time to the end of Bic-CAB treatment and OS.
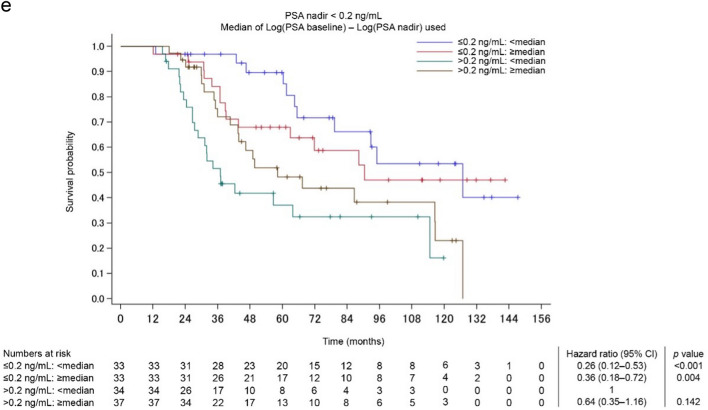
Results: The median observation period was 46.4 months, and the median age of patients at diagnosis was 71 years. A total of 46.5% patients experienced PSA progression with a median survival duration of 29 months (according to Prostate Cancer Clinical Trials Working Group 3 criteria), and 49.1% patients achieved a PSA nadir < 0.2 ng/mL in a median time of 4.7 months. When stratified by PSA nadir and PSA change, patients at low risk for disease progression with a small PSA change due to low initial PSA had a 5-year OS of 100% and a 10-year OS of 75%. The OS during the observation period was 72.9 months.
Conclusion: These findings highlight the potential effect of Bic-CAB in patients with mHSPC who were at low risk for disease progression. Initial treatment with Bic-CAB and adjusting treatment early based on PSA dynamics may be a reasonable treatment plan for these patients.
Keywords: Bicalutamide; Combined androgen blockage; Japan; Metastatic hormone-sensitive prostate cancer.
© 2024. The Author(s).
Conflict of interest statement
Yu Tashiro, Kentaro Ueno, Naoki Terada, Takuya Hida, and Ryoma Kurahashi have no conflict of interest. Shusuke Akamatsu has received honoraria and research funding from Astellas Pharma Inc. Toshiyuki Kamoto has received honoraria from Janssen Pharmaceuticals, AstraZeneca, Sanofi, and Takeda; received research funding from EP CRSU Company Limited, MSD, Bayer Yakuhin Limited, and AstraZeneca; and scholarship funding from Takeda and Shin Nippon Biomedical Laboratories. Tomomi Kamba has received honoraria from Takeda, AstraZeneca, and Merck Biopharma. Atsushi Saito and Takumi Lee are employees of Astellas Pharma Inc. Satoshi Morita has received honoraria from AstraZeneca, Astellas Pharma Inc, Bristol Myers Squibb, Chugai, Eisai, Elli Lily, MSD, and Ono. Takashi Kobayashi has received honoraria from Astellas Pharma Inc, Janssen, and Bayer.
Figures


References
-
- Sung H, Ferlay J, Siegel RL et al (2021) Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71:209–249 - PubMed
-
- Center for Cancer Control and Information Services (2022) Available via Cancer Statistics in Japan. https://ganjoho.jp/reg_stat/statistics/stat/cancer/20_prostate.html. Accessed Feb 2024
-
- Parker C, Castro E, Fizazi K et al (2020) Prostate cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 31:1119–1134 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
