

Epidemiology, ventilation management and outcomes of COVID-19 ARDS patients versus patients with ARDS due to pneumonia in the Pre-COVID era
- PMID: 39153979
- PMCID: PMC11330602
- DOI: 10.1186/s12931-024-02910-2
Epidemiology, ventilation management and outcomes of COVID-19 ARDS patients versus patients with ARDS due to pneumonia in the Pre-COVID era
Erratum in
-
Correction to: Epidemiology, ventilation management and outcomes of COVID-19 ARDS patients versus patients with ARDS due to pneumonia in the Pre-COVID era.Respir Res. 2025 Mar 28;26(1):117. doi: 10.1186/s12931-025-03176-y. Respir Res. 2025. PMID: 40155913 Free PMC article. No abstract available.
Abstract
Background: Ventilation management may differ between COVID-19 ARDS (COVID-ARDS) patients and patients with pre-COVID ARDS (CLASSIC-ARDS); it is uncertain whether associations of ventilation management with outcomes for CLASSIC-ARDS also exist in COVID-ARDS.
Methods: Individual patient data analysis of COVID-ARDS and CLASSIC-ARDS patients in six observational studies of ventilation, four in the COVID-19 pandemic and two pre-pandemic. Descriptive statistics were used to compare epidemiology and ventilation characteristics. The primary endpoint were key ventilation parameters; other outcomes included mortality and ventilator-free days and alive (VFD-60) at day 60.
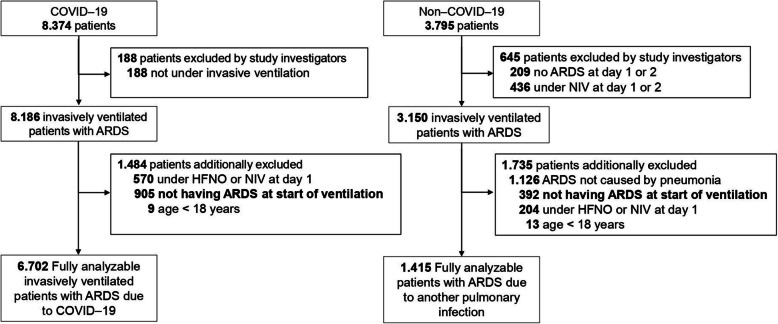
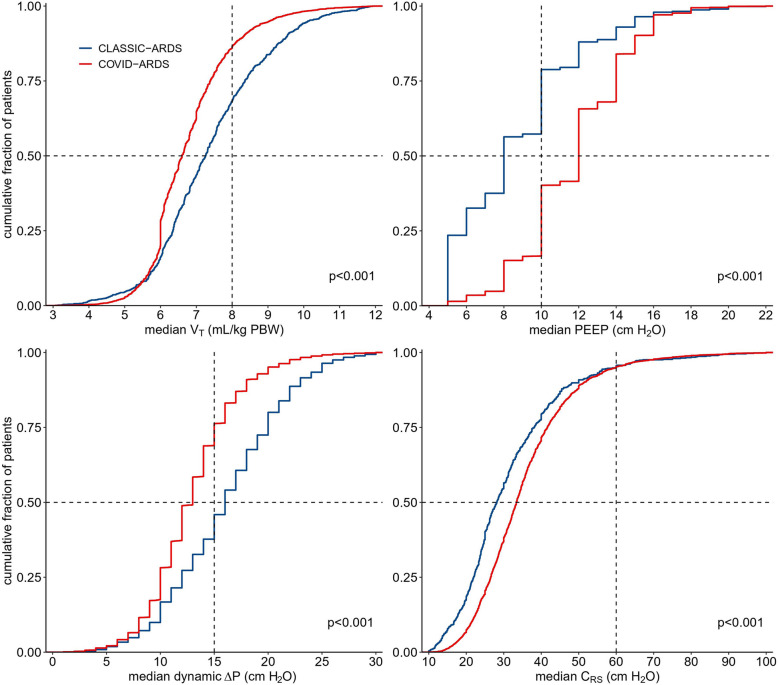
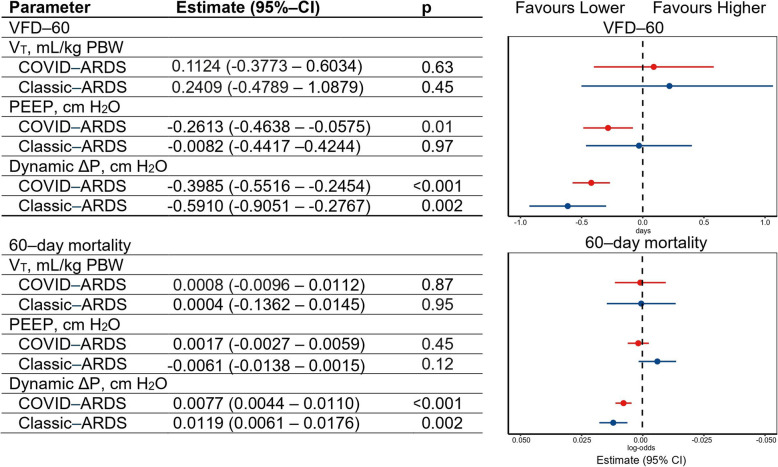
Results: This analysis included 6702 COVID-ARDS patients and 1415 CLASSIC-ARDS patients. COVID-ARDS patients received lower median VT (6.6 [6.0 to 7.4] vs 7.3 [6.4 to 8.5] ml/kg PBW; p < 0.001) and higher median PEEP (12.0 [10.0 to 14.0] vs 8.0 [6.0 to 10.0] cm H2O; p < 0.001), at lower median ΔP (13.0 [10.0 to 15.0] vs 16.0 [IQR 12.0 to 20.0] cm H2O; p < 0.001) and higher median Crs (33.5 [26.6 to 42.1] vs 28.1 [21.6 to 38.4] mL/cm H2O; p < 0.001). Following multivariable adjustment, higher ΔP had an independent association with higher 60-day mortality and less VFD-60 in both groups. Higher PEEP had an association with less VFD-60, but only in COVID-ARDS patients.
Conclusions: Our findings show important differences in key ventilation parameters and associations thereof with outcomes between COVID-ARDS and CLASSIC-ARDS.
Trial registration: Clinicaltrials.gov (identifier NCT05650957), December 14, 2022.
Keywords: ARDS; Acute respiratory distress syndrome; COVID–19; Critical care; Mechanical ventilation; Ventilation management.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Chiumello D, Busana M, Coppola S, Romitti F, Formenti P, Bonifazi M, Pozzi T, Palumbo MM, Cressoni M, Herrmann P, Meissner K, Quintel M, Camporota L, Marini JJ, Gattinoni L. Physiological and quantitative CT-scan characterization of COVID-19 and typical ARDS: a matched cohort study. Intensive Care Med. 2020;46:2187–96. - PMC - PubMed
-
- Grasselli G, Tonetti T, Protti A, Langer T, Girardis M, Bellani G, Laffey J, Carrafiello G, Carsana L, Rizzuto C, Zanella A, Scaravilli V, Pizzilli G, Grieco DL, Di Meglio L, de Pascale G, Lanza E, Monteduro F, Zompatori M, Filippini C, Locatelli F, Cecconi M, Fumagalli R, Nava S, Vincent JL, Antonelli M, Slutsky AS, Pesenti A, Ranieri VM. Pathophysiology of COVID-19-associated acute respiratory distress syndrome: a multicentre prospective observational study. Lancet Respir Med. 2020;8:1201–8. - PMC - PubMed
-
- Grasselli G, Zangrillo A, Zanella A, Antonelli M, Cabrini L, Castelli A, Cereda D, Coluccello A, Foti G, Fumagalli R, Iotti G, Latronico N, Lorini L, Merler S, Natalini G, Piatti A, Ranieri MV, Scandroglio AM, Storti E, Cecconi M, Pesenti A. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020;323:1574–81. - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
