

Multiplex real-time PCR in non-invasive respiratory samples to reduce antibiotic use in community-acquired pneumonia: a randomised trial
- PMID: 39154071
- PMCID: PMC11330507
- DOI: 10.1038/s41467-024-51547-8
Multiplex real-time PCR in non-invasive respiratory samples to reduce antibiotic use in community-acquired pneumonia: a randomised trial
Abstract
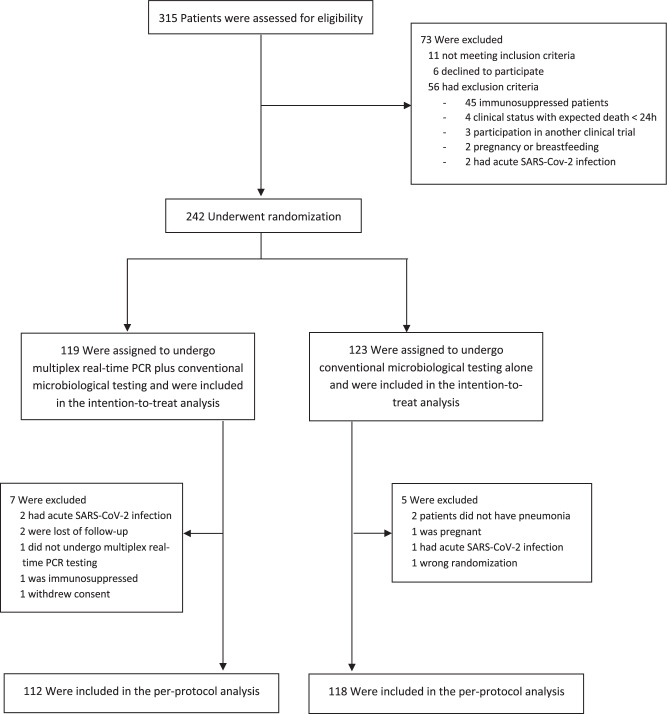
We assessed whether multiplex real-time PCR plus conventional microbiological testing is safe and more effective than conventional microbiological testing alone for reducing antibiotic use in community-acquired pneumonia (CAP). In this randomised trial, we recruited adults hospitalised with CAP at four Spanish hospitals. Patients were randomly assigned (1:1) to undergo either multiplex real-time PCR in non-invasive respiratory samples plus conventional microbiological testing or conventional microbiological testing alone. The primary endpoint was antibiotic use measured by days of antibiotic therapy (DOT). Between February 20, 2020, and April 24, 2023, 242 patients were enrolled; 119 were randomly assigned to multiplex real-time PCR plus conventional microbiological testing and 123 to conventional microbiological testing alone. All but one of the patients allocated to multiplex real-time PCR plus conventional microbiological testing underwent PCR, which was performed in sputum samples in 77 patients (65.2%) and in nasopharyngeal swabs in 41 (34.7%). The median DOT was 10.04 (IQR 7.98, 12.94) in the multiplex PCR plus conventional microbiological testing group and 11.33 (IQR 8.15, 16.16) in the conventional microbiological testing alone group (difference -1.04; 95% CI, -2.42 to 0.17; p = 0.093). No differences were observed in adverse events and 30-day mortality. Our findings do not support the routine implementation of multiplex real-time PCR in the initial microbiological testing in hospitalised patients with CAP. Clinicaltrials.gov registration: NCT04158492.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Metlay, J. P. et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med.200, e45–e67 (2019). 10.1164/rccm.201908-1581ST - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
