

PSMA-PET/CT response after metastasis-directed radiotherapy of bone oligometastases in prostate cancer
- PMID: 39155339
- PMCID: PMC11330950
- DOI: 10.1186/s41824-024-00212-w
PSMA-PET/CT response after metastasis-directed radiotherapy of bone oligometastases in prostate cancer
Abstract
Objective: Bone metastases are very common in advanced prostate cancer and can sensitively be detected utilizing PSMA-PET/CT. Therefore, our goal was to evaluate the suitability of PSMA-PET/CT-guided metastasis-directed external beam radiotherapy (MDT) as treatment option for patients with biochemical recurrence and oligometastatic bone lesions.
Materials & methods: We retrospectively examined 32 prostate cancer patients with biochemical recurrence and PSMA-positive oligometastatic disease limited to the bone (n = 1-3). A total of 49 bone lesions were treated with MDT. All patients received a post-radiotherapy PSMA-PET/CT-Scan. Changes in SUVmax, PSMA-positive tumor volume per lesion and PSA, as well as the correlation between the PET/CT-interval and SUVmax response were calculated.
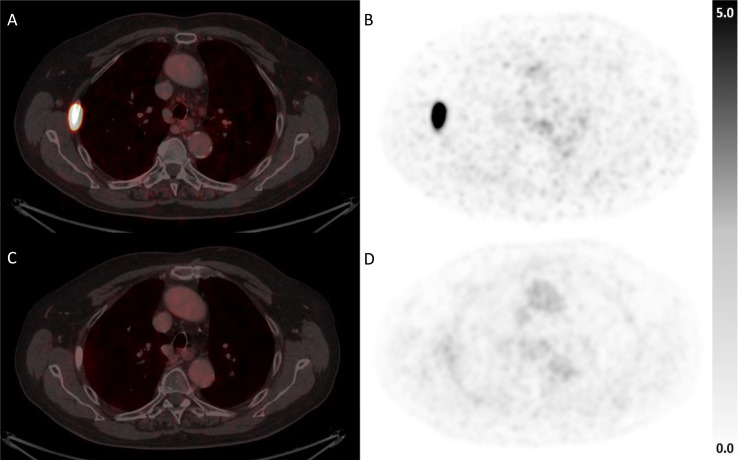
Results: MDT lead to a SUVmax decrease in 46/49 (94%) of the lesions. The median relative decline of SUVmax was 60.4%, respectively. Based on PSMA-positive lesion volume with a SUV cut-off of 4, 46/49 (94%) of lesions showed complete response, two (4%) partial response and one lesion (2%) was stable on PSMA-PET/CT after MDT. Most of the treated patients (56.3%) showed an initial PSA decline at three months and a PSA nadir of median 0.14 ng/ml after a median time of 3.6 months after MDT. The median relative PSA change at three months after MDT was 3.9%.
Conclusion: MDT is a very effective treatment modality for prostate cancer bone oligometastases and lesion response to MDT can be assessed using the (semi-)quantitative parameters SUVmax and PSMA-positive lesion volume with established SUV cut-offs.
Keywords: Metastases directed therapy (MDT); Oligometastatic prostate cancer (OMPC); PET/CT; Prostate specific membrane antigen (PSMA); Response assessment.
© 2024. The Author(s).
Conflict of interest statement
Lena M. Unterrainer received personal fees from Novartis Radiopharmaceuticals, Astellas Pharma Inc., Telix Pharmaceuticals and is on the advisory board of Telix Pharmaceuticals. All other authors declare that they have no conflicts of interest or competing interests.
Figures


References
-
- Anderson EM, McBride SM (2022) The Use of Androgen Deprivation Therapy in Combination with Radiation for localized prostate Cancer. Front Urol 2:890814 10.3389/fruro.2022.890814 - DOI
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous