

Anthropometric measures and long-term mortality in non-ischaemic heart failure with reduced ejection fraction: Questioning the obesity paradox
- PMID: 39155576
- PMCID: PMC11955318
- DOI: 10.1002/ejhf.3424
Anthropometric measures and long-term mortality in non-ischaemic heart failure with reduced ejection fraction: Questioning the obesity paradox
Abstract
Aims: Although body mass index (BMI) is the most commonly used anthropometric measure to assess adiposity, alternative indices such as the waist-to-height ratio may better reflect the location and amount of ectopic fat as well as the weight of the skeleton.
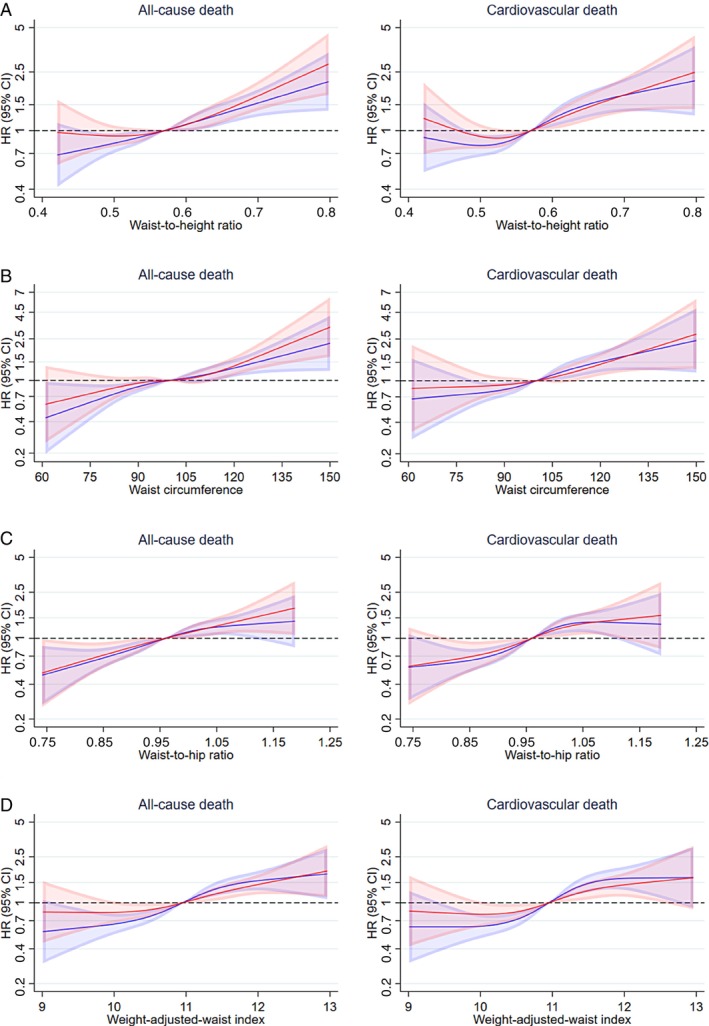
Methods and results: The prognostic value of several alternative anthropometric measures was compared with that of BMI in 1116 patients with non-ischaemic heart failure with reduced ejection fraction (HFrEF) enrolled in DANISH. The association between anthropometric measures and all-cause death was adjusted for prognostic variables, including natriuretic peptides. Median follow-up was 9.5 years (25th-75th percentile, 7.9-10.9). Compared to patients with a BMI 18.5-24.9 kg/m2 (n = 363), those with a BMI ≥25 kg/m2 had a higher risk of all-cause and cardiovascular death, although this association was only statistically significant for a BMI ≥35 kg/m2 (n = 91) (all-cause death: hazard ratio [HR] 1.78, 95% confidence interval [CI] 1.28-2.48; cardiovascular death: HR 2.46, 95% CI 1.69-3.58). Compared to a BMI 18.5-24.9 kg/m2, a BMI <18.5 kg/m2 (n = 24) was associated with a numerically, but not a significantly, higher risk of all-cause and cardiovascular death. Greater waist-to-height ratio (as an exemplar of indices not incorporating weight) was also associated with a higher risk of all-cause and cardiovascular death (HR for the highest vs. the lowest quintile: all-cause death: HR 2.11, 95% CI 1.53-2.92; cardiovascular death: HR 2.17, 95% CI 1.49-3.15).
Conclusion: In patients with non-ischaemic HFrEF, there was a clear association between greater adiposity and higher long-term mortality.
Clinical trial registration: ClinicalTrials.gov NCT00542945.
Keywords: Anthropometric measures; Body mass index; Clinical trial; Heart failure with reduced ejection fraction.
© 2024 The Author(s). European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures


References
-
- Lopez‐Jimenez F, Almahmeed W, Bays H, Cuevas A, Di Angelantonio E, le Roux CW, et al. Obesity and cardiovascular disease: Mechanistic insights and management strategies. A joint position paper by the World Heart Federation and World Obesity Federation. Eur J Prev Cardiol 2022;29:2218–2237. 10.1093/eurjpc/zwac187 - DOI - PubMed
-
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2022;24:4–131. 10.1002/ejhf.2333 - DOI - PubMed
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA Guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022;145:e895–e1032. 10.1161/CIR.0000000000001063 - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
