

Renal and Extrarenal Phenotypes in Patients With HNF1B Variants and Chromosome 17q12 Microdeletions
- PMID: 39156164
- PMCID: PMC11328578
- DOI: 10.1016/j.ekir.2024.05.007
Renal and Extrarenal Phenotypes in Patients With HNF1B Variants and Chromosome 17q12 Microdeletions
Abstract
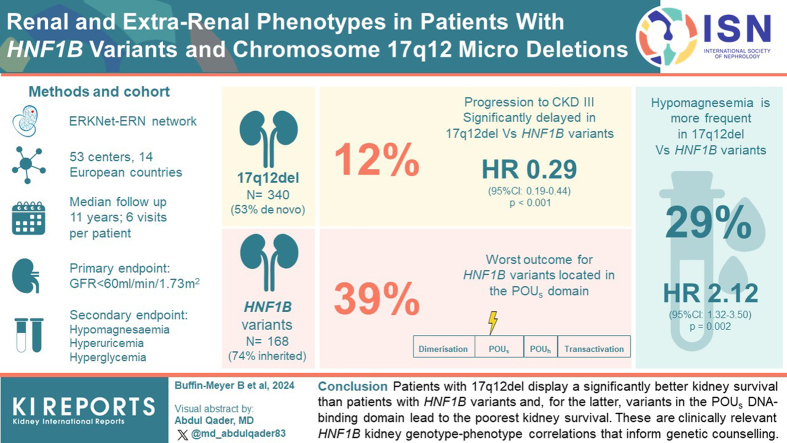
Introduction: Hepatocyte nuclear factor 1-beta (HNF1B) gene variants or the chromosome 17q12 deletion (17q12del) represent the most common monogenic cause of developmental kidney disease. Although neurodevelopmental disorders have been associated with the 17q12del, specific genotype-phenotype associations with respect to kidney function evolution have not yet been fully defined. Here, we aimed to determine whether 17q12del or specific HNF1B variants were associated with kidney survival in a large patient population with HNF1B disease.
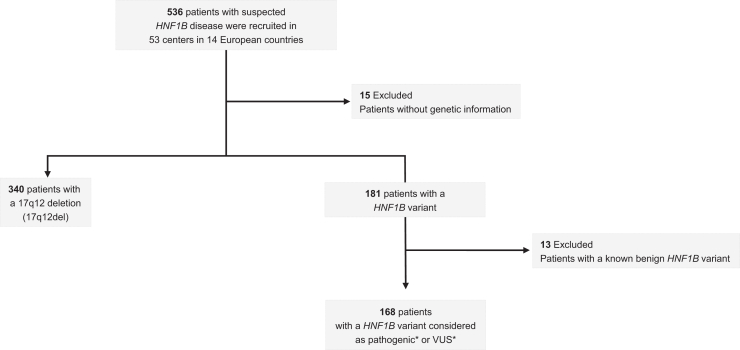
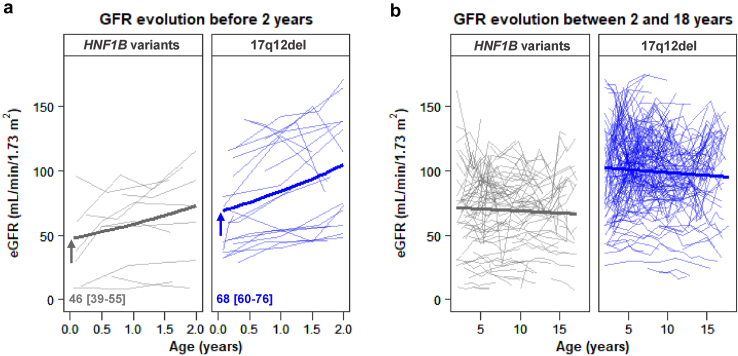
Methods: This was a retrospective observational study involving 521 patients with HNF1B disease from 14 countries using the European Reference Network for rare kidney diseases with detailed information on the HNF1B genotype (HNF1B variants or the 17q12del). Median follow-up time was 11 years with 6 visits per patient. The primary end point was progression to chronic kidney disease (CKD) stage 3 (estimated glomerular filtration rate [eGFR] < 60 ml/min per 1.73 m2). Secondary end points were the development of hypomagnesemia or extrarenal disorders, including hyperuricemia and hyperglycemia.
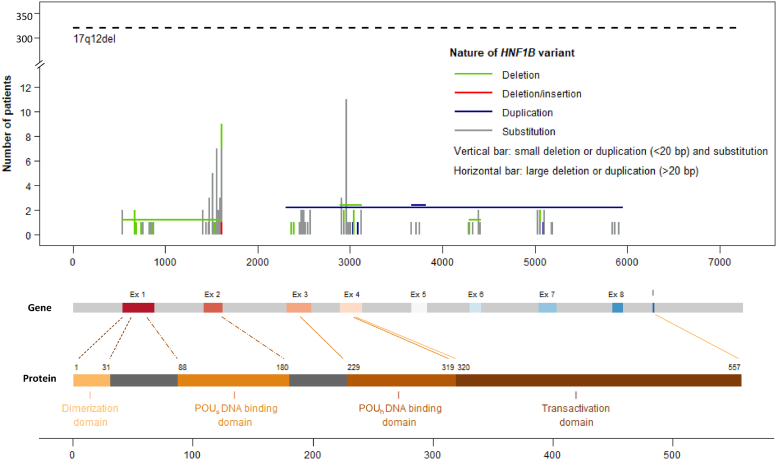
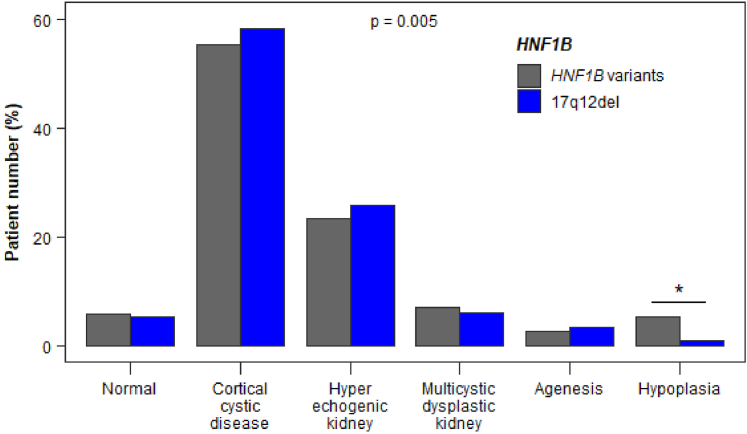
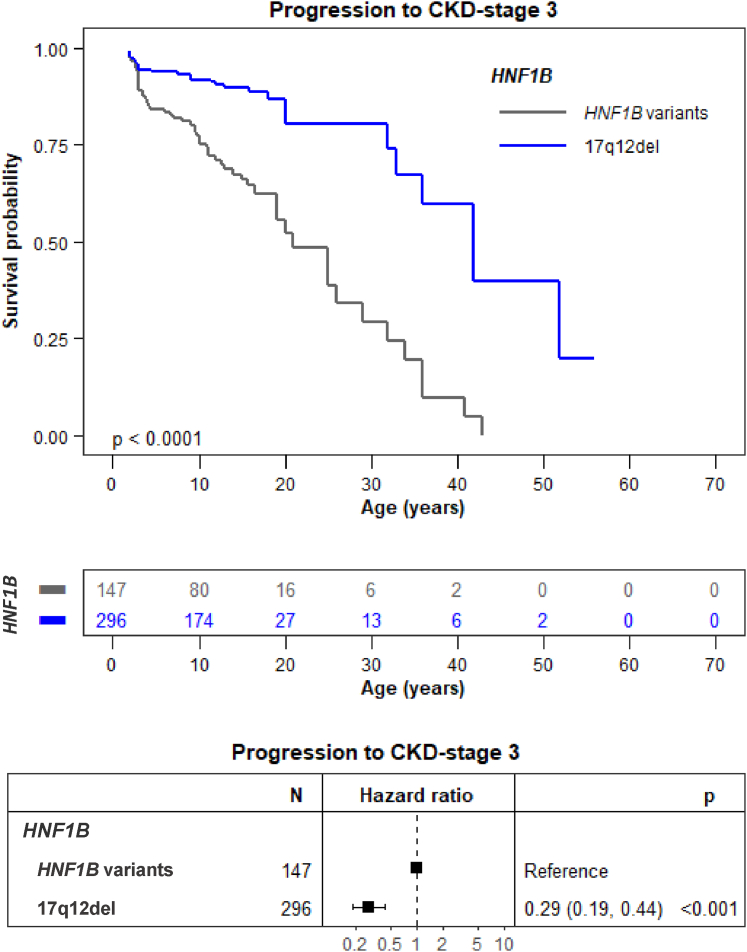
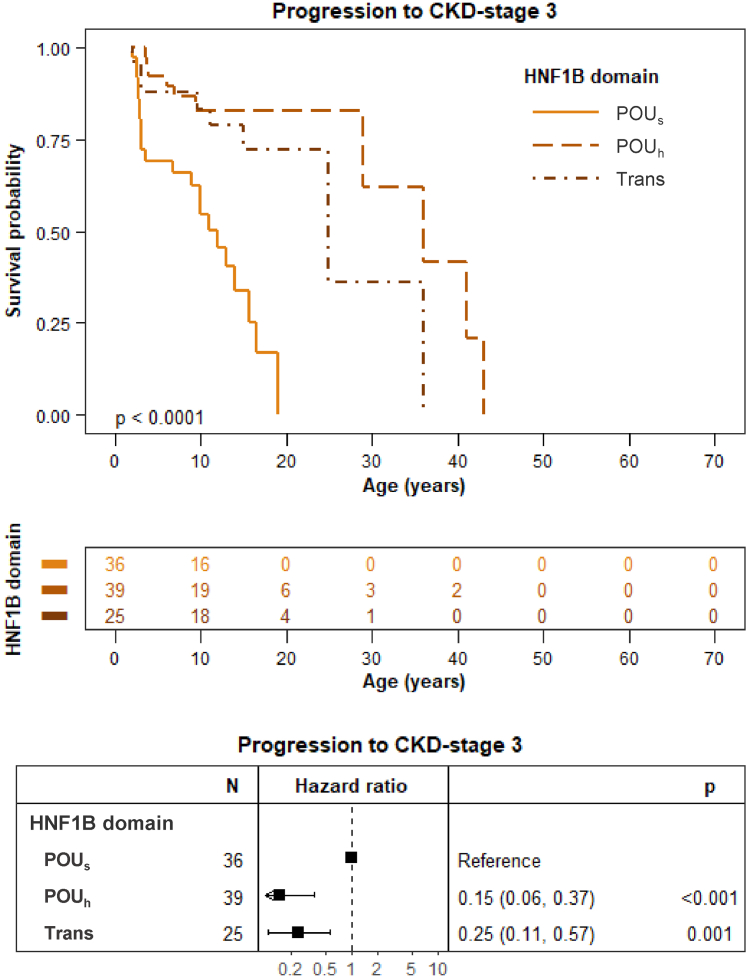
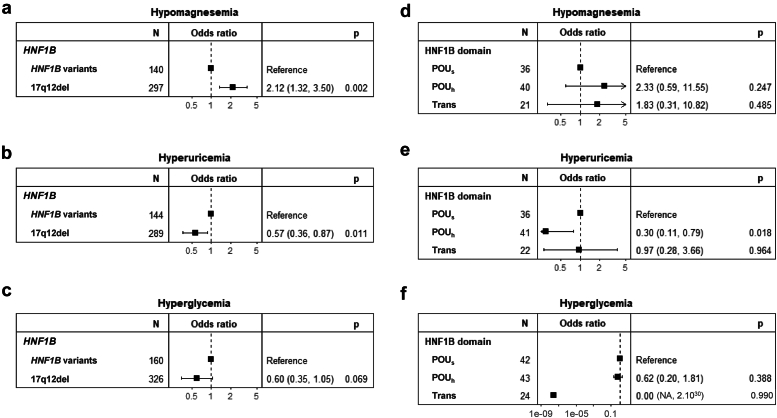
Results: Progression toward CKD stage 3 was significantly delayed in patients with the 17q12del compared to patients with HNF1B variants (hazard ratio [HR]: 0.29, 95% confidence interval [CI]: 0.19-0.44, P < 0.001). Progression toward CKD stage 3 was also significantly delayed when HNF1B variants involved the HNF1B Pit-1, Oct-1, and Unc-86 homeodomain (POUh) DNA-binding and transactivation domains rather than the POU-specific domain (POUs) DNA-binding domain (HR: 0.15 [95% CI: 0.06-0.37), P < 0.001 and HR: 0.25 (95% CI: 0.11-0.57), P = 0.001, respectively). Finally, the 17q12del was positively associated with hypomagnesemia and negatively associated with hyperuricemia, but not with hyperglycemia.
Conclusion: Patients with the 17q12del display a significantly better kidney survival than patients with other HNF1B variants; and for the latter, variants in the POUs DNA-binding domain lead to the poorest kidney survival. These are clinically relevant HNF1B kidney genotype-phenotype correlations that inform genetic counseling.
Keywords: HNF1B disease; chronic kidney disease; genotype-phenotype correlation; outcome.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
