

Clinicopathologic Features of IgG4-Related Kidney Disease
- PMID: 39156178
- PMCID: PMC11328570
- DOI: 10.1016/j.ekir.2024.05.011
Clinicopathologic Features of IgG4-Related Kidney Disease
Abstract
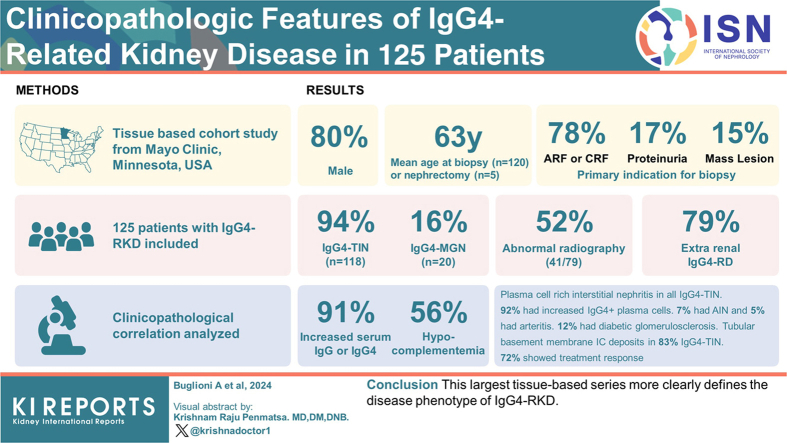
Introduction: IgG4-related disease (IgG4-RD) is a systemic immune-mediated disease that can involve nearly any organ. IgG4-RD can affect the kidney in different disease patterns, collectively referred to as IgG4-related kidney disease (IgG4-RKD).
Methods: We conducted a tissue-based cohort study with clinicopathological correlation in 125 patients with IgG4-RKD.
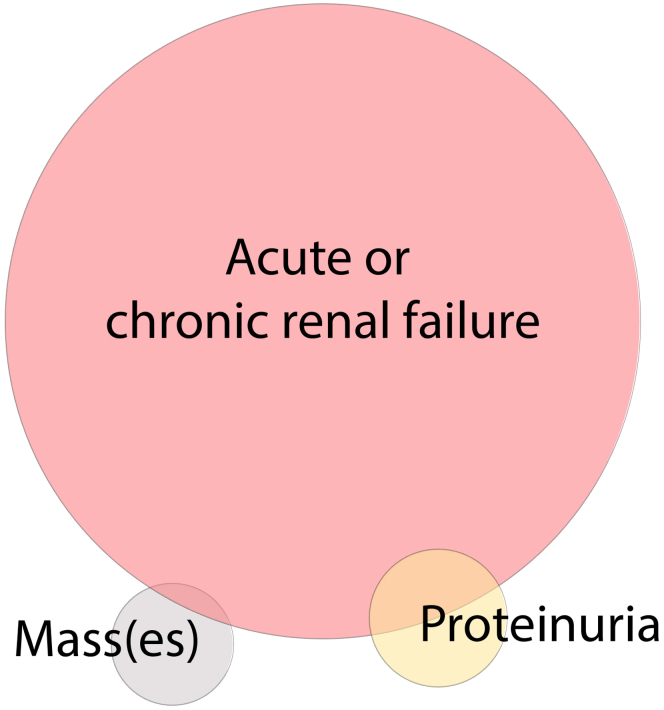
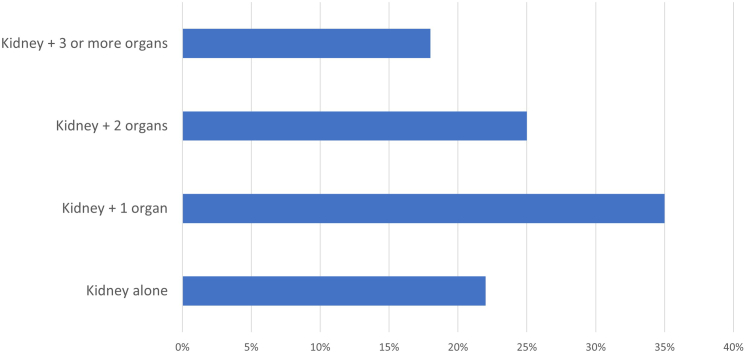
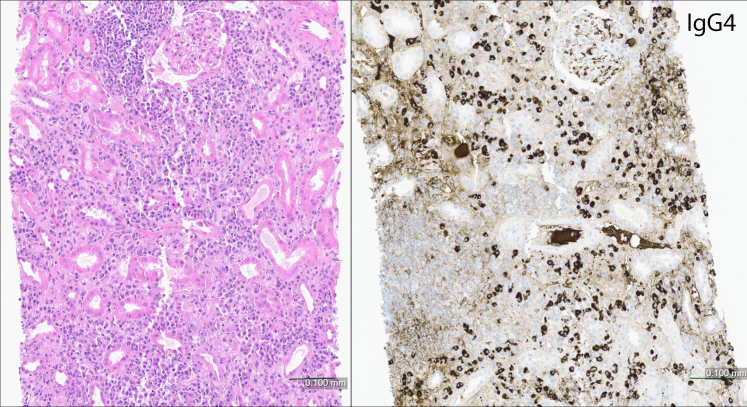
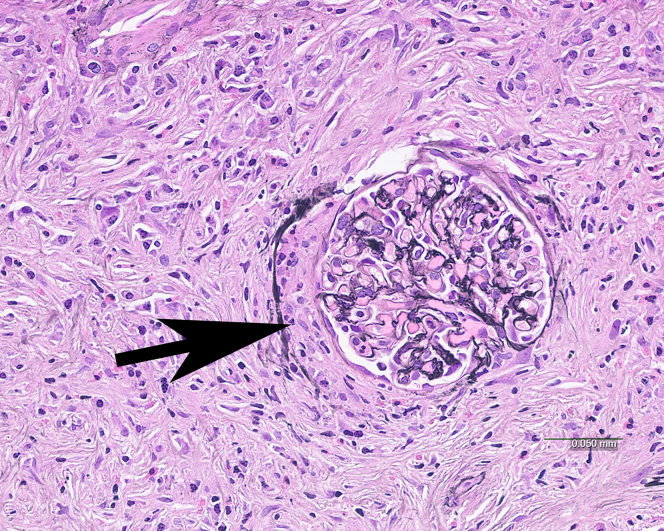
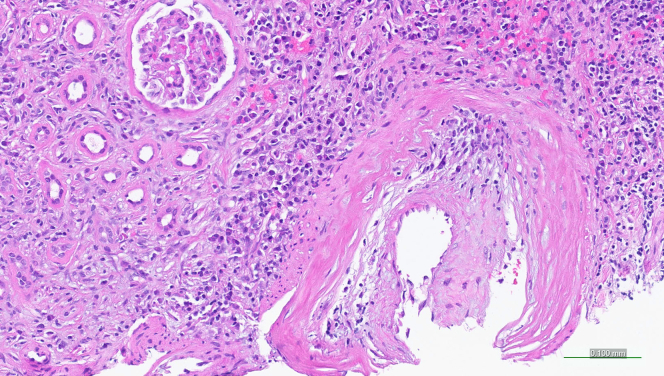
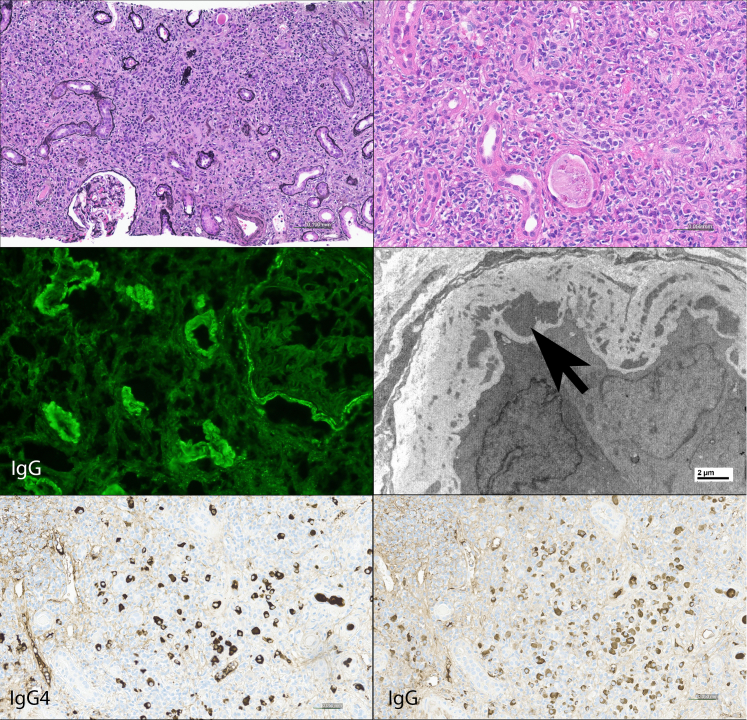
Results: The mean age at biopsy (n = 120) or nephrectomy (n = 5) was 63 years; 80% were male. One hundred eighteen patients (94%) had IgG4-related tubulointerstitial nephritis (IgG4-TIN); 20 patients (16%) had IgG4-related membranous glomerulonephritis (IgG4-MGN; 13 with concurrent IgG4-TIN). The primary clinical indication for biopsy/nephrectomy was acute or chronic renal failure in 78%, proteinuria in 17%, and mass lesion(s) in 15% (with overlap in primary indication). Fifty-two percent patients (41/79) had abnormal radiographic findings, including masses in 30% (24/79). All patients with IgG4-MGN had proteinuria. Extrarenal involvement by IgG4-RD was present in 79%. Median serum creatinine at presentation was 2.5 mg/dl (range 0.7-12). Serum IgG and/or IgG4 was increased in 91% (53/58); hypocomplementemia was present in 56% (43/77). Light microscopy showed plasma cell-rich interstitial nephritis in all cases of IgG4-TIN. Ninety-two percent of patients showed increased IgG4+ plasma cells. Seven percent showed an acute interstitial nephritis (AIN) pattern, and 5% showed non-necrotizing arteritis. Tubular basement membrane immune deposits were present in 83% of IgG4-TIN. Treatment information was available for 71 patients; 62 were treated with immunosuppression. Of those with elevated creatinine, 72% (41/57) showed a treatment response.
Conclusion: This largest tissue-based series more clearly defines the disease phenotype of IgG4-RKD.
Keywords: IgG4-related disease; autoimmune; interstitial nephritis; membranous nephropathy; tubulointerstitial nephritis.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
