

Immune-targeted therapy with transarterial chemo(embolization) for unresectable HCC: a systematic review and meta-analysis
- PMID: 39156893
- PMCID: PMC11329924
- DOI: 10.3389/fimmu.2024.1421520
Immune-targeted therapy with transarterial chemo(embolization) for unresectable HCC: a systematic review and meta-analysis
Abstract
Background: Transarterial chemo(embolization) is preferred for treating unresectable hepatocellular carcinoma (uHCC); however, because of emerging immune-targeted therapies, its efficacy is at stake. This systematic review pioneers to evaluate the clinical efficacy and safety of transarterial chemo(embolization) combined with immune-targeted therapy for uHCC patients.
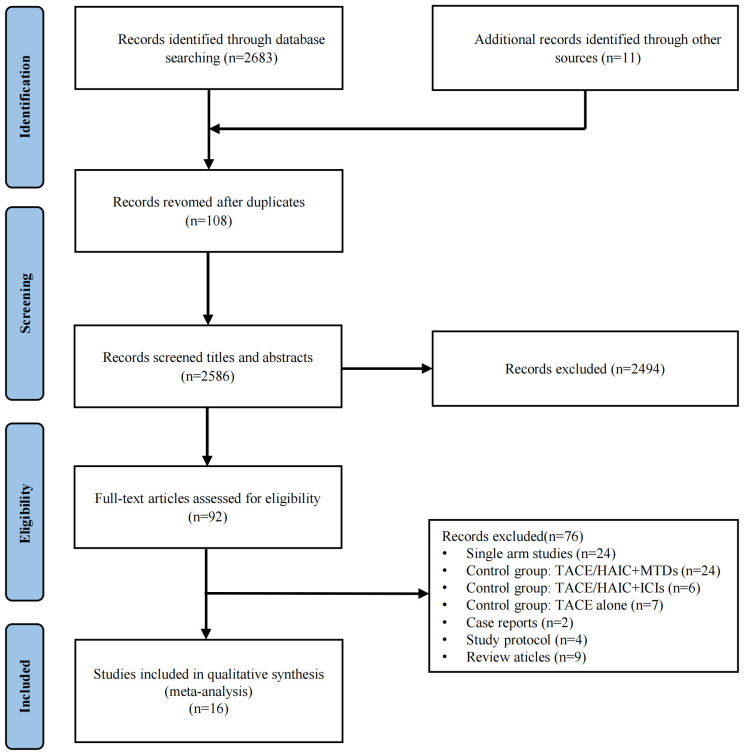
Methods: PubMed, Embase, and Cochrane Library were searched for studies comparing immune-targeted therapy with or without transarterial chemo(embolization) until 31 May 2024. The complete response (CR) rate, objective response rate (ORR), and disease control rate (DCR) were considered to be the primary outcomes calculated for the clinical outcomes of transarterial chemo(embolization) combined with immune-targeted therapy, along with progression-free survival (PFS) and overall survival (OS). The incidence of treatment-related severe adverse events was set as the major measure for the safety outcome.
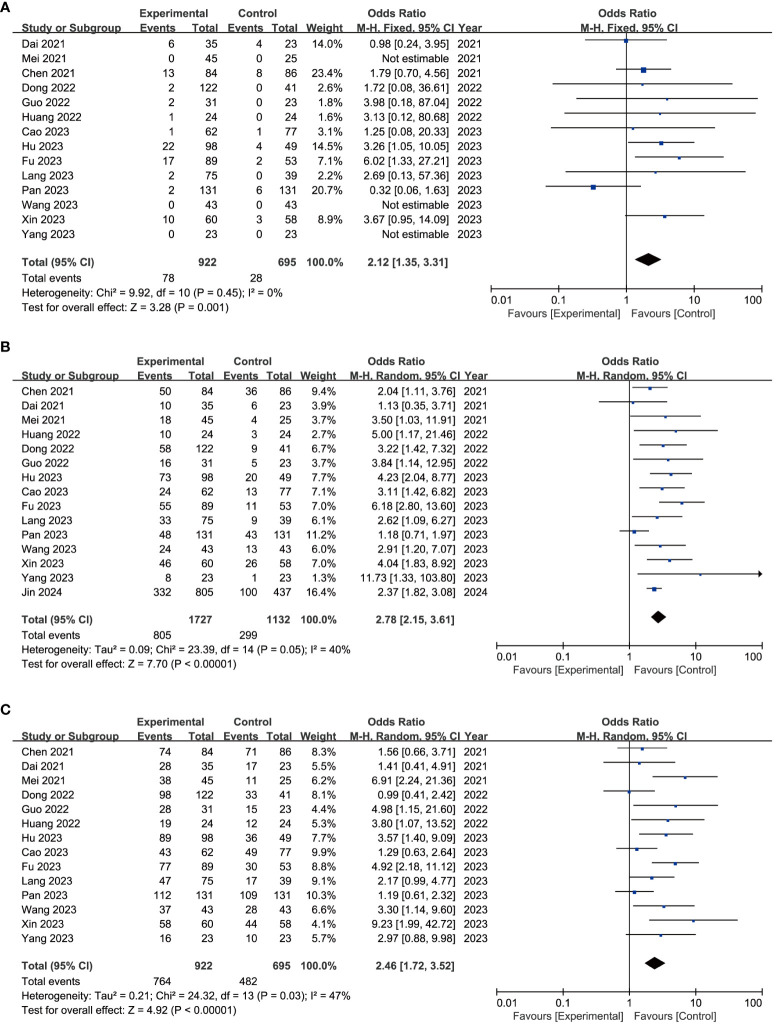
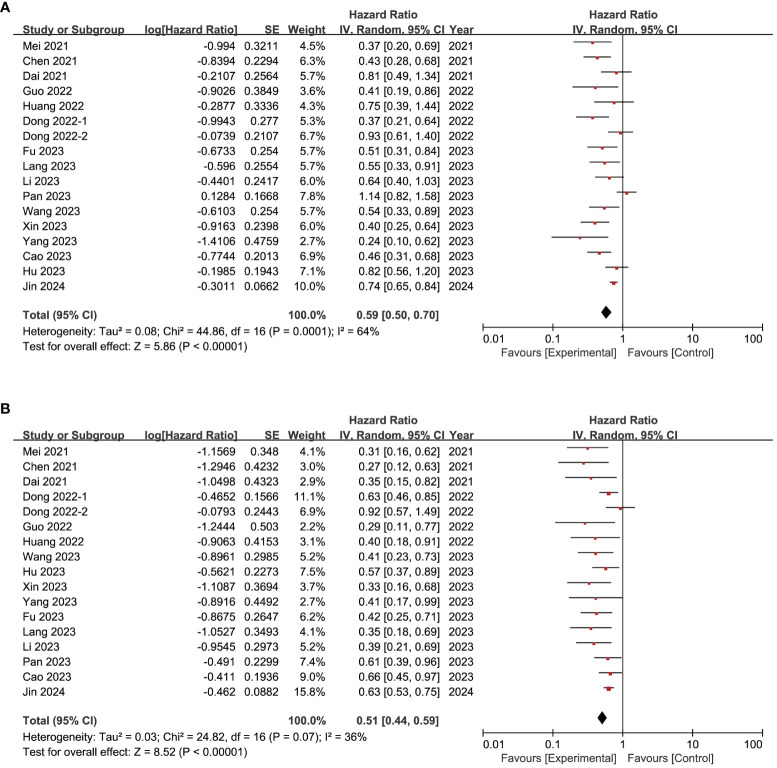
Results: Sixteen studies, encompassing 1,789 patients receiving transarterial chemo(embolization) plus immune-targeted therapy and 1,215 patients receiving immune-targeted therapy alone, were considered eligible. The combination of transarterial chemo(embolization) and immune-targeted therapy demonstrated enhanced outcomes in CR (OR = 2.12, 95% CI = 1.35-3.31), ORR (OR = 2.78, 95% CI = 2.15-3.61), DCR (OR = 2.46, 95% CI = 1.72-3.52), PFS (HR = 0.59, 95% CI = 0.50-0.70), and OS (HR = 0.51, 95% CI = 0.44-0.59), albeit accompanied by a surge in ALT (OR = 2.17, 95% CI = 1.28-3.68) and AST (OR = 2.28, 95% CI = 1.42-3.65). The advantages of additional transarterial chemo(embolization) to immune-targeted therapy were also verified in subgroups of first-line treatment, intervention techniques, with or without extrahepatic metastasis, Child-Pugh grade A or B, and with or without tumor thrombus.
Conclusion: The combination of transarterial chemo(embolization) and immune-targeted therapy seems to bolster local control and long-term efficacy in uHCC, albeit at the expense of hepatic complications.
Systematic review registration: http://www.crd.york.ac.uk/PROSPERO/, identifier 474669.
Keywords: immunotherapy; systematic review; targeted agents; transarterial chemo(embolization); unresectable hepatocellular carcinoma.
Copyright © 2024 Fang, Ke, Wu, Tu and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Xu J, Shen J, Gu S, Zhang Y, Wu L, Wu J, et al. Camrelizumab in combination with apatinib in patients with advanced hepatocellular carcinoma (Rescue): A nonrandomized, open-label, phase ii trial. Clin Cancer Res an Off J Am Assoc Cancer Res. (2021) 27:1003–11. doi: 10.1158/1078-0432.Ccr-20-2571 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical