

Recognition patterns of acute kidney injury in hospitalized patients
- PMID: 39157067
- PMCID: PMC11328729
- DOI: 10.1093/ckj/sfae231
Recognition patterns of acute kidney injury in hospitalized patients
Abstract
Background: Acute kidney injury (AKI) during hospitalization is associated with increased complications and mortality. Despite efforts to standardize AKI management, its recognition in clinical practice is limited.
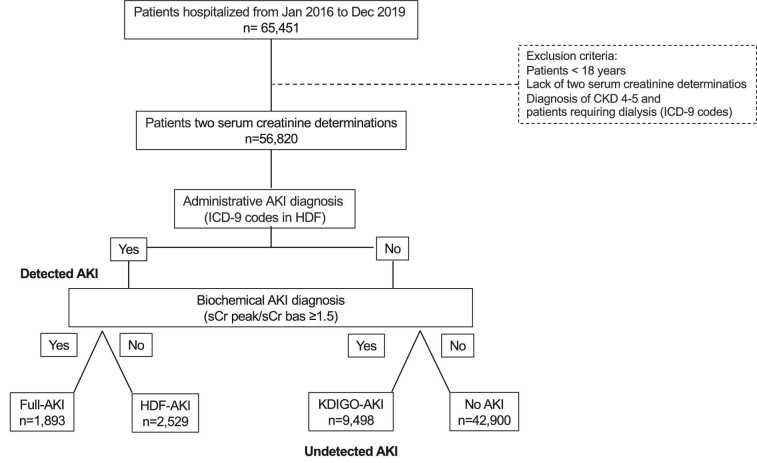
Methods: To assess and characterize different patterns of AKI diagnosis, we collected clinical data, serum creatinine (sCr) levels, comorbidities and outcomes from adult patients using the Hospital Discharge Form (HDF). AKI diagnosis was based on administrative data and according to Kidney Disease: Improving Global Outcomes (KDIGO) criteria by evaluating sCr variations during hospitalization. Additionally, patients were categorized based on the timing of AKI onset.
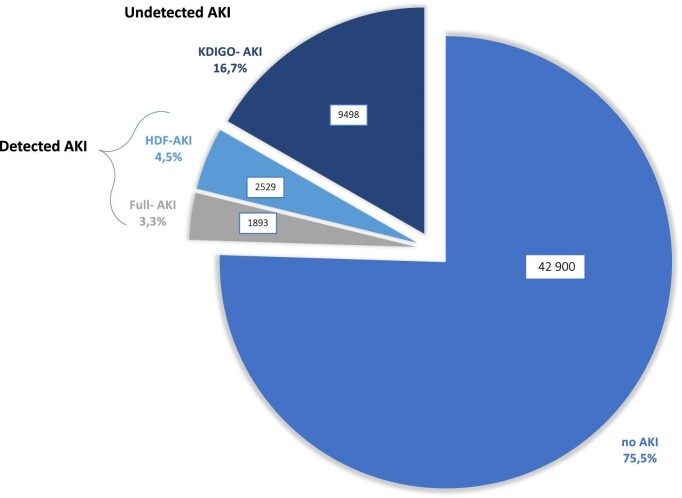
Results: Among 56 820 patients, 42 900 (75.5%) had no AKI, 1893 (3.3%) had AKI diagnosed by sCr changes and coded in the HDF (full-AKI), 2529 (4.4%) had AKI reported on the HDF but not meeting sCr-based criteria (HDF-AKI) and 9498 (16.7%) had undetected AKI diagnosed by sCr changes but not coded in the HDF (KDIGO-AKI). Overall, AKI incidence was 24.5%, with a 68% undetection rate. Patients with KDIGO-AKI were younger and had a higher proportion of females, lower comorbidity burden, milder AKI stages, more frequent admissions to surgical wards and lower mortality compared with full-AKI patients. All AKI groups had worse outcomes than those without AKI, and AKI, even if undetected, was independently associated with mortality risk. Patients with AKI at admission had different profiles and better outcomes than those developing AKI later.
Conclusions: AKI recognition in hospitalized patients is highly heterogeneous, with a significant prevalence of undetection. This variability may be affected by patients' characteristics, AKI-related factors, diagnostic approaches and in-hospital patient management. AKI remains a major risk factor, emphasizing the importance of ensuring proper diagnosis for all patients.
Keywords: AKI; administrative data; diagnosis; mortality; serum creatinine.
© The Author(s) 2024. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
LinkOut - more resources
Full Text Sources
