

Optimal Management for Primary High Grade Ta Bladder Cancer: Role of re-staging TURBT and Intravesical Adjuvant Therapy
- PMID: 39157168
- PMCID: PMC11327485
- DOI: 10.1002/bco2.363
Optimal Management for Primary High Grade Ta Bladder Cancer: Role of re-staging TURBT and Intravesical Adjuvant Therapy
Erratum in
-
Erratum.BJUI Compass. 2024 Dec 30;5(12):1324-1329. doi: 10.1002/bco2.482. eCollection 2024 Dec. BJUI Compass. 2024. PMID: 39744071 Free PMC article.
Abstract
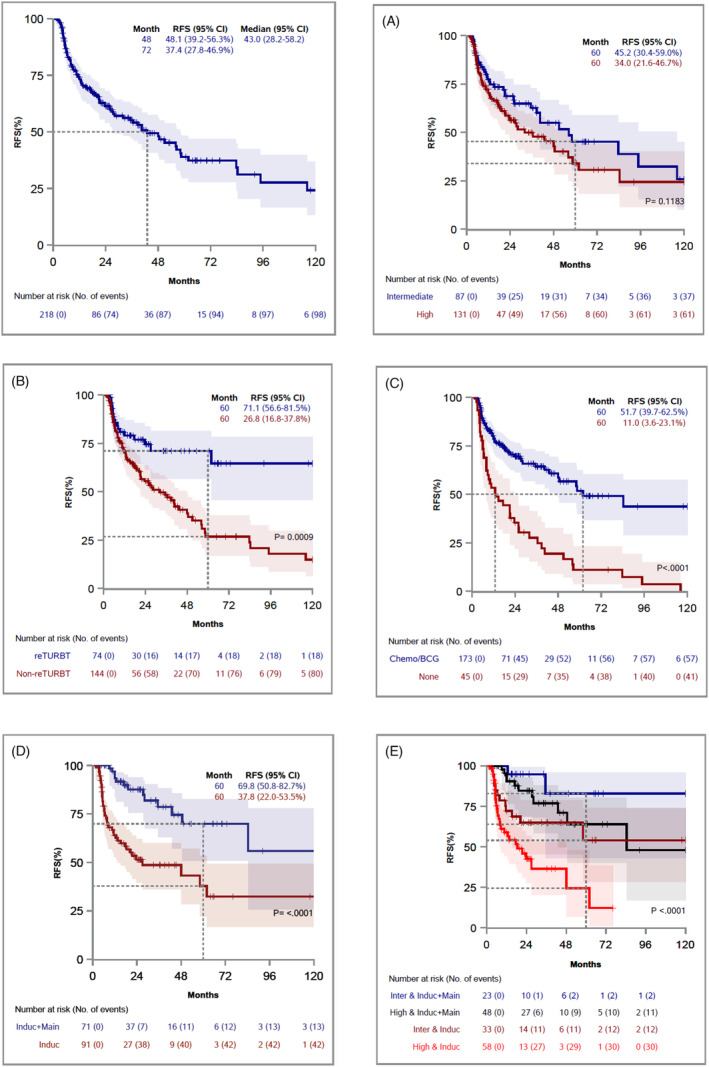
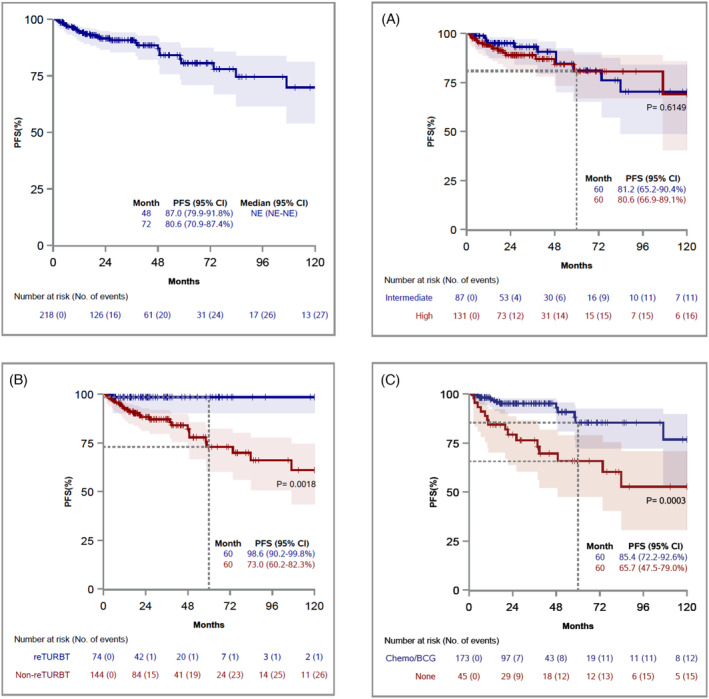
Objective: This study aims to investigate the impact of risk group classification, restaging transurethral resection (re-TURBT), and adjuvant treatment intensity on recurrence and progression risks in high-grade Ta tumours in patients with non-muscle invasive bladder cancer (NMIBC).
Materials and methods: Data from a comprehensive bladder cancer database were utilized for this study. Patients with primary high-grade Ta tumours were included. Risk groups were classified according to AUA/SUO criteria. Tumour characteristics and patient demographics were analysed using descriptive statistics. Cox proportional hazard regression models were used to assess the effect of re-TURBT and other clinical/treatment-related predictors on recurrence- and progression-free survivals. The survivals by selected predictors were estimated using Kaplan-Meier method, and groups were compared by the log-rank test.
Results: Among 218 patients with high-grade Ta bladder cancer, those who underwent re-TURBT had significantly better 5-year recurrence-free survival (71.1% vs. 26.8%, p = 0.0009) and progression-free survival (98.6% vs. 73%, p = 0.0018) compared with those with initial TURBT alone. Full BCG treatment (induction and maintenance) showed lower recurrence risk, especially in high-risk patients. However, residual disease at re-TURBT did not significantly affect recurrence risk.
Conclusions: This study highlights the significance of risk group classification, the role of re-TURBT, and the intensity of adjuvant treatment in the management of high-grade Ta tumours. A risk-adapted model is crucial to reduce the burden of unnecessary intravesical treatment and endoscopic procedures.
Keywords: non‐muscle invasive bladder cancer; progression‐free survival; recurrence‐free survival; restaging transurethral resection of bladder tumour.
© 2024 The Authors. BJUI Compass published by John Wiley & Sons Ltd on behalf of BJU International Company.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Gontero P, Compérat E, Dominguez JL, Liedberg F, Masson‐Lecomte A, Mostafid AH, et al. Non‐muscle‐invasive Bladder Cancer (TaT1 and CIS) EAU Guidelines on 2023.
-
- Cumberbatch MGK, Foerster B, Catto JWF, Kamat AM, Kassouf W, Jubber I, et al. Repeat Transurethral Resection in Non–muscle‐invasive Bladder Cancer: A Systematic Review [Figure presented], European Urology 73 Elsevier B.V.; 2018. p. 925–933. - PubMed
LinkOut - more resources
Full Text Sources