

Management of greater tuberosity fracture dislocations of the shoulder
- PMID: 39157260
- PMCID: PMC11329025
- DOI: 10.1016/j.xrrt.2023.07.007
Management of greater tuberosity fracture dislocations of the shoulder
Abstract
Background: Despite extensive literature dedicated to determining the optimal treatment of isolated greater tuberosity (GT) fractures, there have been few studies to guide the management of GT fracture dislocations. The purpose of this review was to highlight the relevant literature pertaining to all aspects of GT fracture dislocation evaluation and treatment.
Methods: A narrative review of the literature was performed.
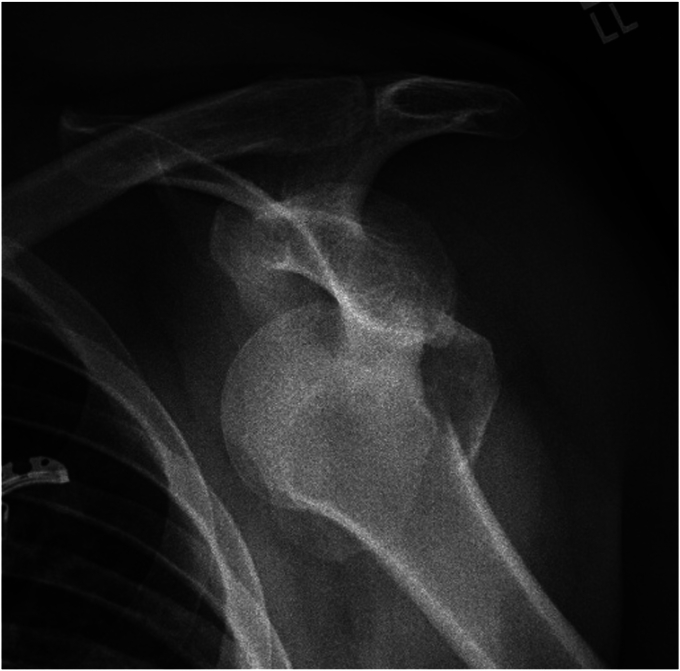
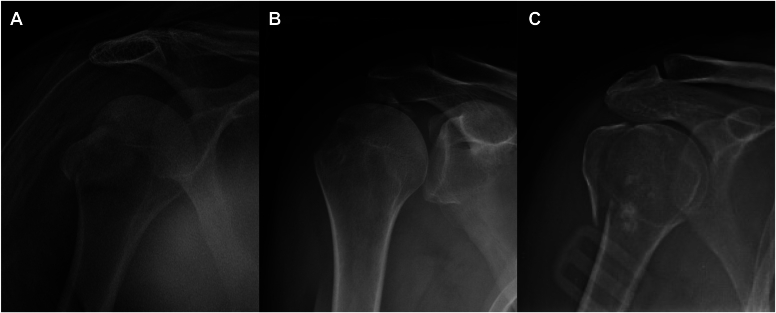
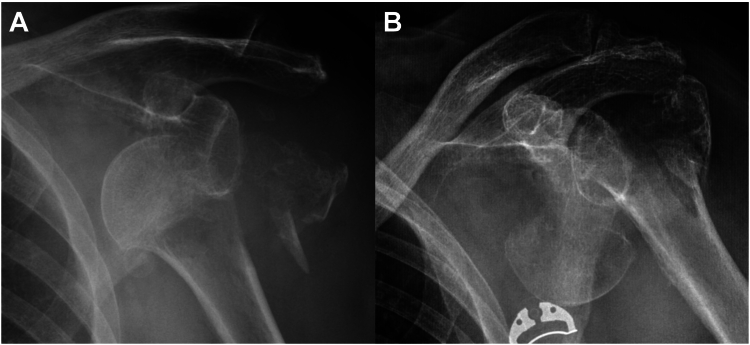
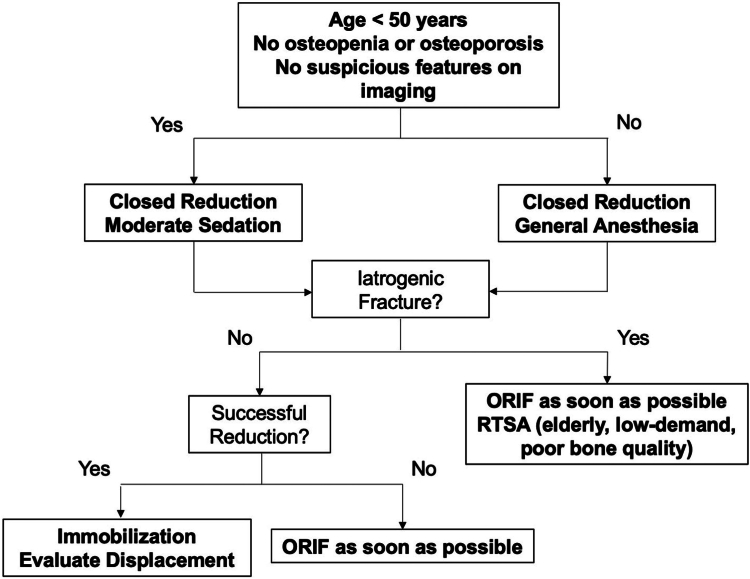
Results: During glenohumeral reduction, an iatrogenic humeral neck fracture may occur due to the presence of an occult neck fracture or forceful reduction attempts with inadequate muscle relaxation. Minimally displaced GT fragments after shoulder reduction can be successfully treated nonoperatively, but close follow-up is needed to monitor for secondary displacement of the fracture. Surgery is indicated for fractures with >5 mm displacement to minimize the risk of subacromial impingement and altered rotator cuff biomechanics. Multiple surgical techniques have been described and include both open and arthroscopic approaches. Strategies for repair include the use of transosseous sutures, suture anchors, tension bands, screws, and plates. Good-to-excellent radiographic and clinical outcomes can be achieved with appropriate treatment.
Conclusions: GT fracture dislocations of the proximal humerus represent a separate entity from their isolated fracture counterparts in their evaluation and treatment. The decision to employ a certain strategy should depend on fracture morphology and comminution, bone quality, and displacement.
Keywords: Fixation strategies; Fracture dislocation; Greater tuberosity; Iatrogenic fracture; Proximal humerus fracture; Surgical fixation.
© 2023 The Author(s).
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
