

Rate control or rhythm control in patients with atrial fibrillation and acute coronary syndrome or percutaneous coronary intervention
- PMID: 39157410
- PMCID: PMC11328096
- DOI: 10.1016/j.heliyon.2024.e35218
Rate control or rhythm control in patients with atrial fibrillation and acute coronary syndrome or percutaneous coronary intervention
Abstract
Background: Restoring and maintaining sinus rhythm in patients with atrial fibrillation (AF) and acute coronary syndrome (ACS) or undergoing percutaneous coronary intervention (PCI) has been studied in clinical trials to reduce symptoms and improve quality of life. Limited data exist on the effectiveness of rate or rhythm control therapy in these patients.
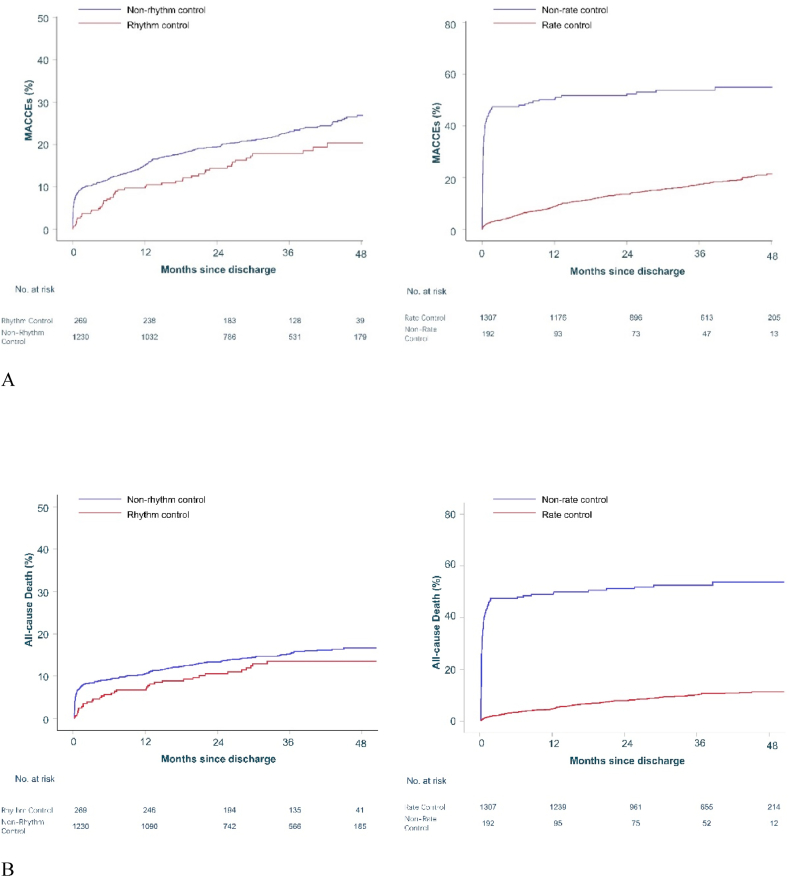
Methods: Consecutive patients with AF and ACS or referred for PCI were prospectively recruited in Fuwai Hospital during 2017-2020. The primary endpoints were all-cause death and major adverse cardiovascular and cerebrovascular events (MACCEs), including cardiovascular mortality, myocardial infarction, ischemic stroke, non-central nervous system embolism and ischemia-driven revascularization. Kaplan-Meier curves and Cox regressions were performed to evaluate the association between rhythm/rate control and subsequent outcomes. For the primary endpoints, we used the Benjamini-Hochberg correction for multiple comparisons.
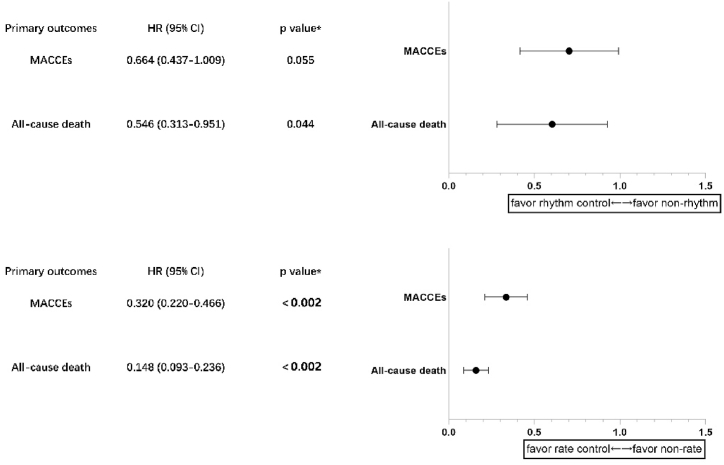
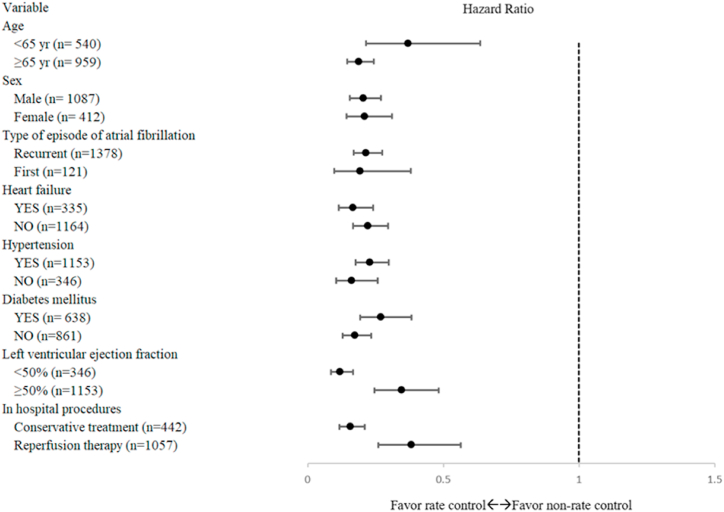
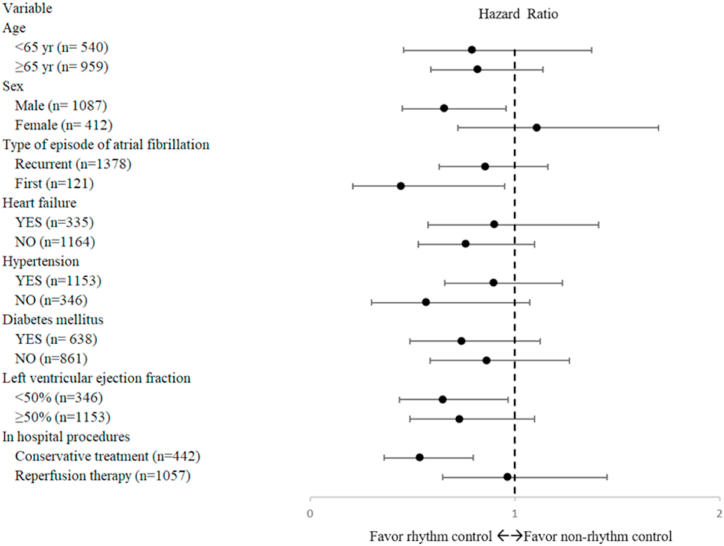
Results: A total of 1499 patients with AF and ACS or undergoing PCI were included, with a median follow-up of 34.7 months. Compared to non-rate control, rate control strategy reduced the risk of subsequent MACCEs (adjusted HR, 0.320; 95 % CI 0.220-0.466; p <0.001; *p <0.002) and all-cause death (adjusted HR, 0.148; 95 % CI 0.093-0.236; p <0.001; *p <0.002). Similar trends were observed across all predefined subgroups (p <0.001). In the final multivariate model, rhythm control was not associated with a lower subsequent MACCEs but significantly improved all-cause mortality compared to non-rhythm control (adjusted HR, 0.546; 95 % CI 0.313-0.951; p =0.033; *p =0.044).
Conclusions: In this real-world study, rate control strategy was associated with lower risk of MACCEs and all-cause death in AF and ACS or undergoing PCI. Besides, management with rhythm control strategy may improve all-cause mortality.
Keywords: Acute coronary syndrome; Atrial fibrillation; Rate control; Rhythm control.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Eisen A., Giugliano R.P., Braunwald E. Updates on acute coronary syndrome: a review. JAMA Cardiology. 2016;1:718–730. - PubMed
-
- Crijns H.J., Van Gelder I.C., Van Gilst W.H., Hillege H., Gosselink A.M., Lie K.I. Serial antiarrhythmic drug treatment to maintain sinus rhythm after electrical cardioversion for chronic atrial fibrillation or atrial flutter. Am. J. Cardiol. 1991;68:335–341. - PubMed
-
- Krahn A.D., Manfreda J., Tate R.B., Mathewson F.A., Cuddy T.E. The natural history of atrial fibrillation: incidence, risk factors, and prognosis in the Manitoba Follow-Up Study. Am. J. Med. 1995;98:476–484. - PubMed
-
- Baseline characteristics of patients with atrial fibrillation: the AFFIRM Study. Am. Heart J. 2002;143:991–1001. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
