

Assessing the arrhythmogenic propensity of fibrotic substrate using digital twins to inform a mechanisms-based atrial fibrillation ablation strategy
- PMID: 39157719
- PMCID: PMC11329066
- DOI: 10.1038/s44161-024-00489-x
Assessing the arrhythmogenic propensity of fibrotic substrate using digital twins to inform a mechanisms-based atrial fibrillation ablation strategy
Abstract
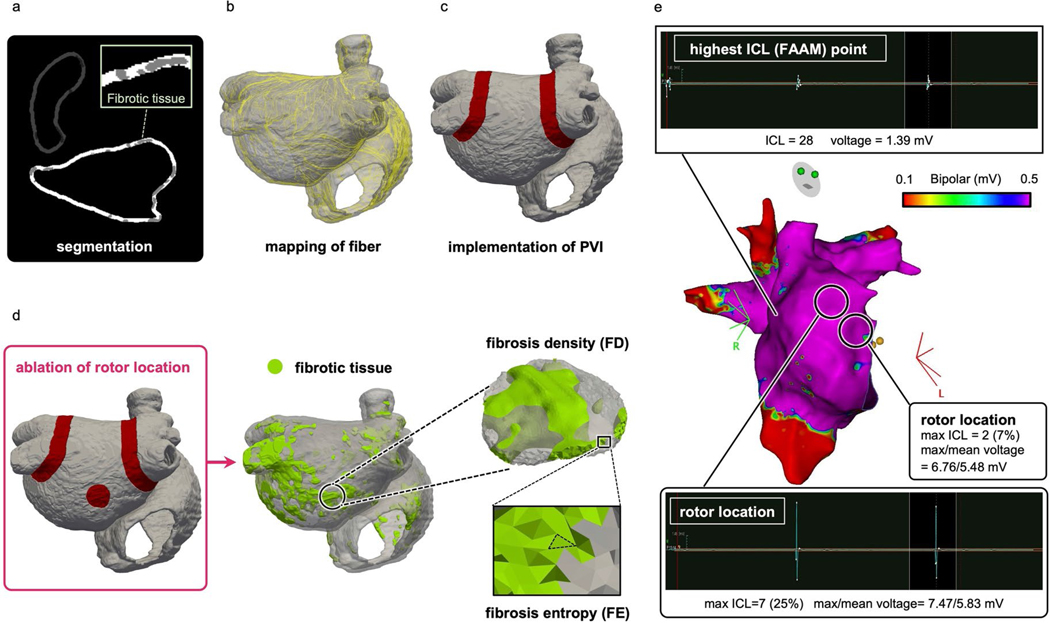
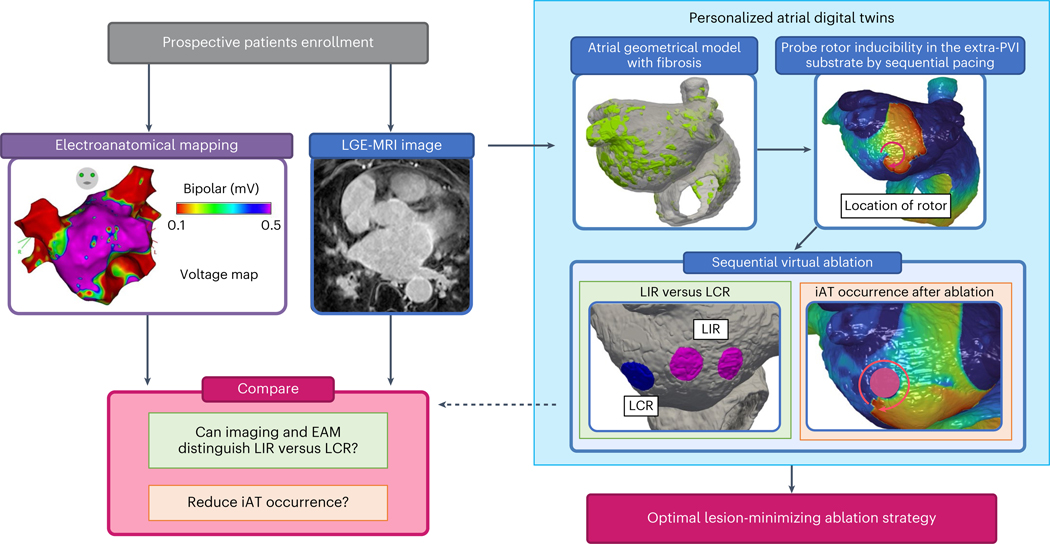
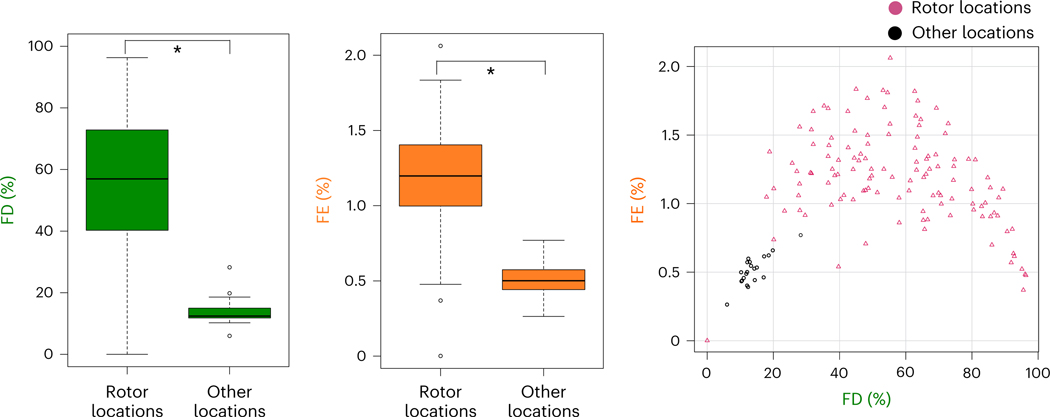
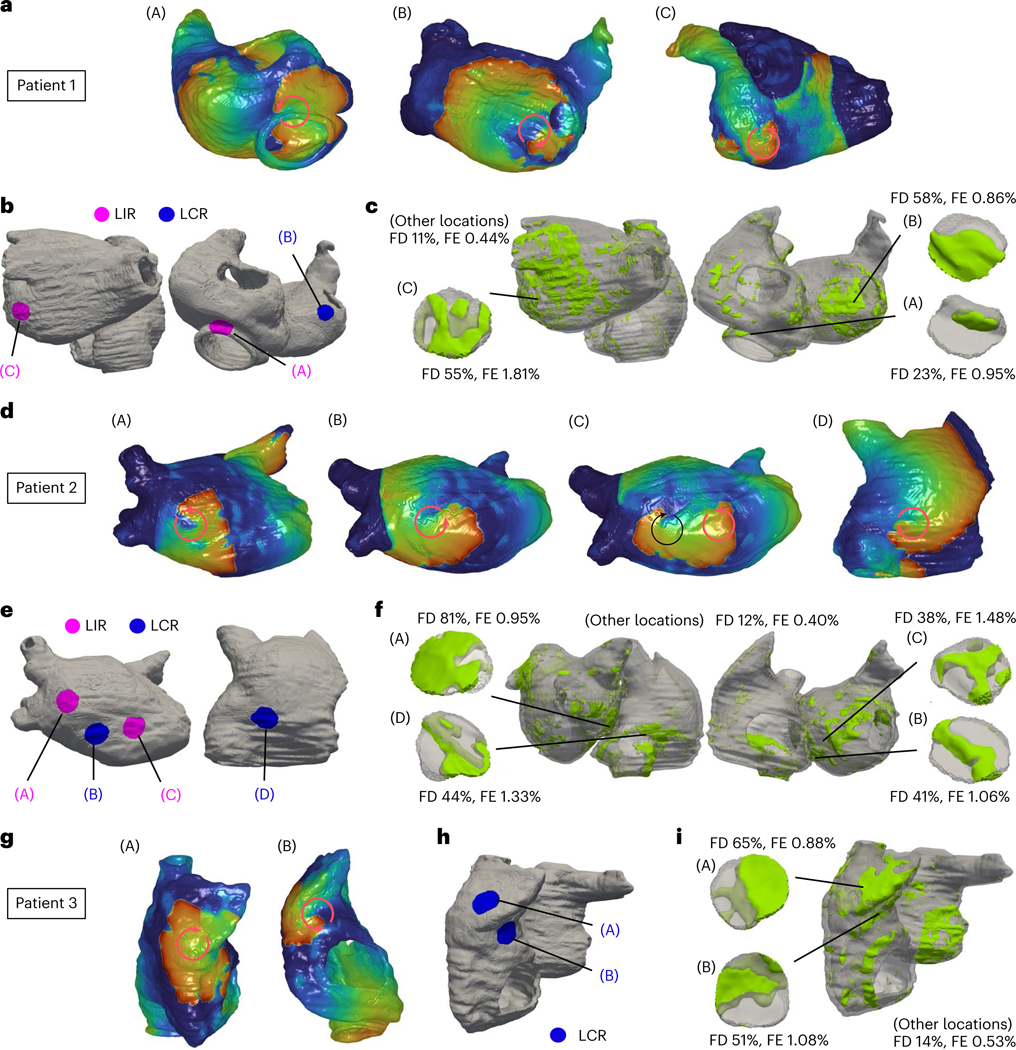
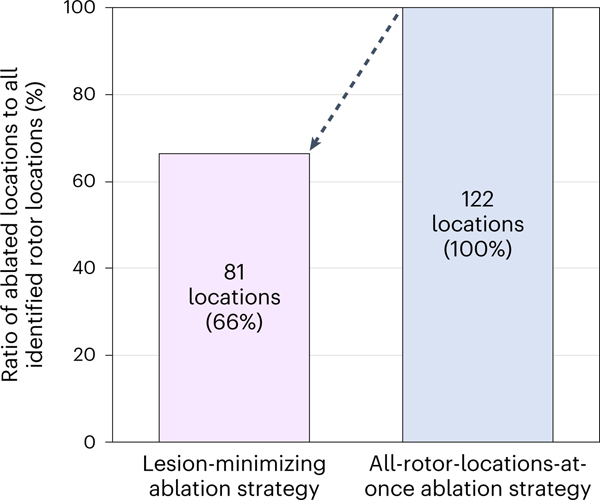
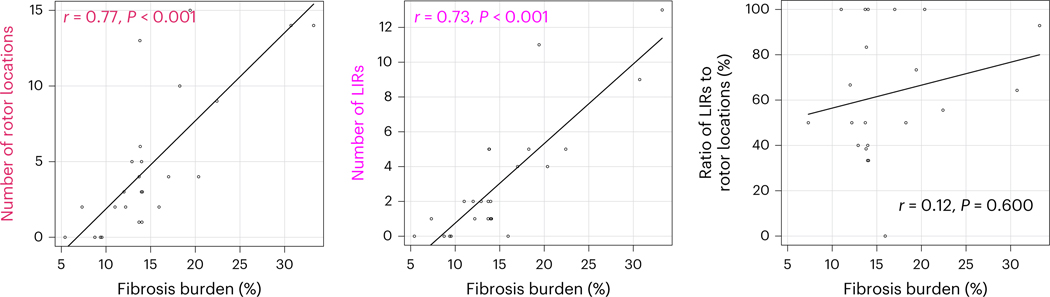
Atrial fibrillation (AF), the most common heart rhythm disorder, may cause stroke and heart failure. For patients with persistent AF with fibrosis proliferation, the standard AF treatment-pulmonary vein isolation-has poor outcomes, necessitating redo procedures, owing to insufficient understanding of what constitutes good targets in fibrotic substrates. Here we present a prospective clinical and personalized digital twin study that characterizes the arrhythmogenic properties of persistent AF substrates and uncovers locations possessing rotor-attracting capabilities. Among these, a portion needs to be ablated to render the substrate not inducible for rotors, but the rest (37%) lose rotor-attracting capabilities when another location is ablated. Leveraging digital twin mechanistic insights, we suggest ablation targets that eliminate arrhythmia propensity with minimum lesions while also minimizing the risk of iatrogenic tachycardia and AF recurrence. Our findings provide further evidence regarding the appropriate substrate ablation targets in persistent AF, opening the door for effective strategies to mitigate patients' AF burden.
Figures
References
-
- Haïssaguerre M. et al. Electrophysiological breakthroughs from the left atrium to the pulmonary veins. Circulation 102, 2463–2465 (2000). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources