

Favorable safety profile of NOAC therapy in patients after tricuspid transcatheter edge-to-edge repair
- PMID: 39158599
- PMCID: PMC12202579
- DOI: 10.1007/s00392-024-02517-z
Favorable safety profile of NOAC therapy in patients after tricuspid transcatheter edge-to-edge repair
Abstract
Background: Transcatheter edge-to-edge repair for severe tricuspid regurgitation (TR) is a new treatment option (t-TEER). Data on optimal antithrombotic therapy after t-TEER in patients with an indication for anticoagulation are scarce and evidence-based guideline recommendations are lacking. We sought to investigate efficacy and safety of novel oral anticoagulation (NOAC) and vitamin-K-antagonists (VKA) in patients undergoing t-TEER.
Methods: Among 78 consecutive patients with t-TEER of severe TR, 69 patients were identified with concomitant indication for oral anticoagulation. Outcomes of these patients treated with NOAC or VKA were compared over a median follow-up period of 327 (177-460) days.
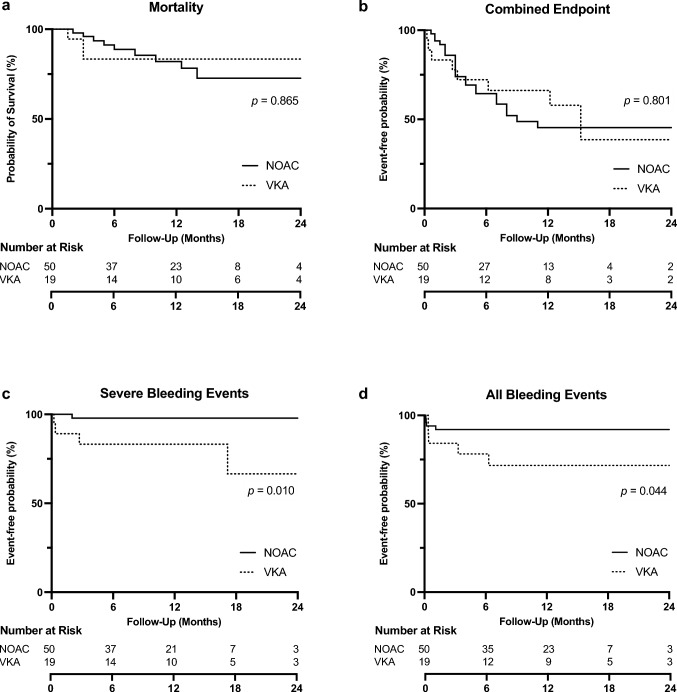
Results: Despite elevated thromboembolic and bleeding risk scores (CHA2DS2-VASc 4.2 ± 1.1, HEMORR2HAGES 3.0 ± 1.0 and HAS-BLED 2.1 ± 0.8), only one major bleeding incidence occurred under NOAC therapy. The risk for overall (NOAC 8% vs. VKA group 26%, p = 0.044) and major bleeding events (NOAC 2% vs. VKA 21%, p = 0.010) was significantly lower in the NOAC compared to the VKA group. No significant difference was found between NOAC and VKA treatment in terms of mortality (NOAC 18% vs. VKA 16%, p = 0.865) or the combined endpoint of death, heart failure hospitalization, stroke, embolism, thrombosis, myocardial infarction, and severe bleeding (NOAC 48% vs. VKA 42%, p = 0.801). A comparison between apixaban (n = 27) and rivaroxaban (n = 16) treated patients revealed no significant differences between NOAC substances (all bleeding events apixaban 7% vs. rivaroxaban 13%, p = 0.638).
Conclusion: Results of this study indicate that NOACs may offer a favorable risk-benefit profile for patients with concomitant indication for anticoagulation therapy following t-TEER.
Keywords: Bleeding; NOAC; Oral anticoagulation; Transcatheter edge-to-edge repair; Transcatheter tricuspid valve repair; Tricuspid disease; Tricuspid regurgitation.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors report no conflict of interest. Ethics approval: The study is based on the principles outlined in the Declaration of Helsinki. Ethical approval was granted by the local Ethics Committee of the University Heidelberg. Informed consent: All patients gave written informed consent to the procedure and the clinical and scientific use of data.
Figures
References
-
- Arsalan M, Walther T, Smith RL, Grayburn PA (2017) Tricuspid regurgitation diagnosis and treatment. Eur Heart J 38:634–638. 10.1093/eurheartj/ehv487 - PubMed
-
- Topilsky Y, Maltais S, Medina Inojosa J et al (2019) Burden of tricuspid regurgitation in patients diagnosed in the community setting. JACC Cardiovasc Imag 12:433–442. 10.1016/j.jcmg.2018.06.014 - PubMed
-
- Sorajja P, Whisenant B, Hamid N et al (2023) Transcatheter repair for patients with tricuspid regurgitation. N Engl J Med. 10.1056/NEJMoa2300525 - PubMed
-
- Lurz P, Stephan von Bardeleben R, Weber M et al (2021) Transcatheter edge-to-edge repair for treatment of tricuspid regurgitation. J Am Coll Cardiol 77:229–239. 10.1016/j.jacc.2020.11.038 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
