

Incident Infarcts in Patients With Stroke and Cerebral Small Vessel Disease: Frequency and Relation to Clinical Outcomes
- PMID: 39159417
- PMCID: PMC11361828
- DOI: 10.1212/WNL.0000000000209750
Incident Infarcts in Patients With Stroke and Cerebral Small Vessel Disease: Frequency and Relation to Clinical Outcomes
Abstract
Background and objectives: Factors associated with cerebral small vessel disease (SVD) progression, including incident infarcts, are unclear. We aimed to determine the frequency of incident infarcts over 1 year after minor stroke and their relation to baseline SVD burden, vascular risks, and recurrent stroke and cognitive outcomes.
Methods: We recruited patients with lacunar or nondisabling cortical stroke. After diagnostic imaging, we repeated structural MRI at 3-6 monthly intervals for 12 months, visually assessing incident infarcts on diffusion-weighted imaging or FLAIR. We used logistic regression to determine associations of baseline vascular risks, SVD score, and index stroke subtype with subsequent incident infarcts. We assessed cognitive and functional outcomes at 1 year using Montreal Cognitive Assessment (MoCA) and modified Rankin scale (mRS), adjusting for baseline age, mRS, MoCA, premorbid intelligence, and SVD score.
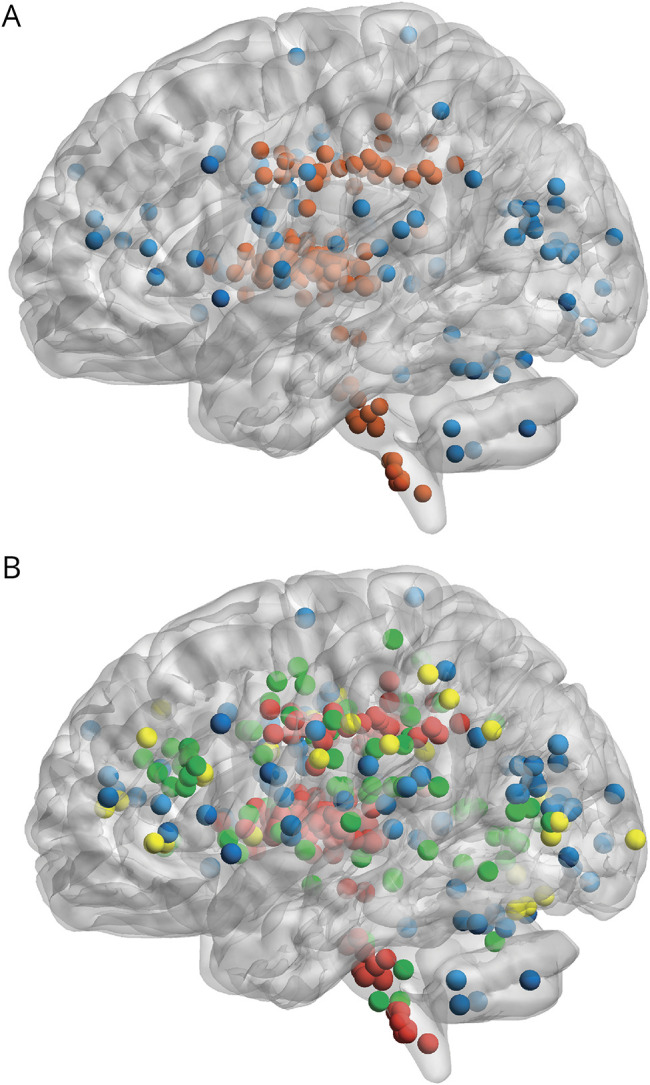
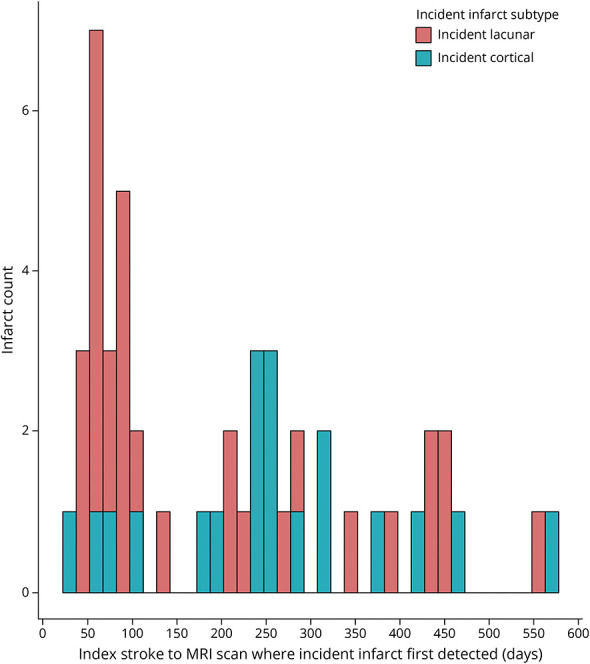
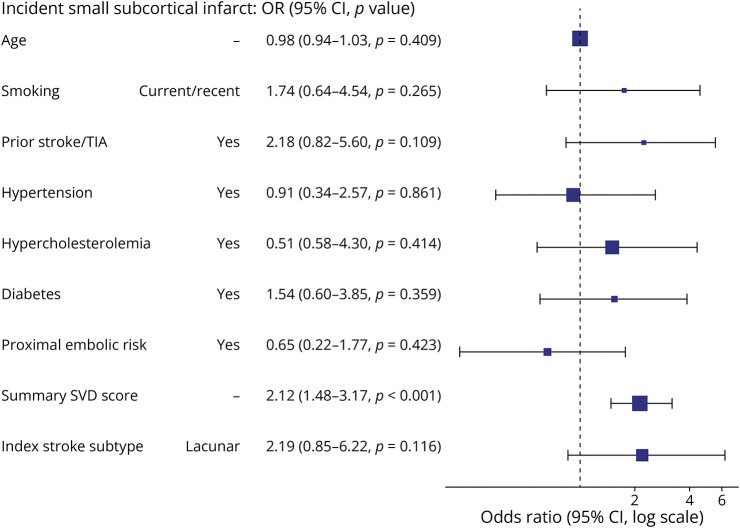
Results: We recruited 229 participants, mean age 65.9 (SD 11.1). Over half of all participants, 131 of 229 (57.2%) had had an index lacunar stroke. From baseline to 1-year MRI, we detected 117 incident infarcts in n = 57/229 (24.8%) participants. Incident infarcts were mainly of the small subcortical (86/117 [73.5%] in n = 38/57 [66.7%]) vs cortical infarct subtype (n = 19/57 [33.3%]). N = 39/57 participants had incident infarcts at 1 visit; 18 of 57 at 2 or more visits; and 19 of 57 participants had multiple infarcts at a single visit. Only 7 of 117 incident infarcts corresponded temporally to clinical stroke syndromes. The baseline SVD score was the strongest predictor of incident infarcts (adjusted odds ratio [OR] 1.87, 95% CI 1.39-2.58), while mean arterial pressure was not associated. All participants with incident infarcts were prescribed an antiplatelet or anticoagulant. Lower 1-year MoCA was associated with lower baseline MoCA (β 0.47, 95% CI 0.33-0.61), lower premorbid intelligence, and older age. Higher 1-year mRS was associated with higher baseline mRS only (OR 5.57 [3.52-9.10]). Neither outcome was associated with incident infarcts.
Discussion: In the year after stroke in a population enriched for lacunar stroke, incident infarcts occurred in one-quarter and were associated with worse baseline SVD. Most incident infarcts detected on imaging did not correspond to clinical stroke/transient ischemic attack. Worse 1-year cognition and function were not associated with incident infarcts.
Conflict of interest statement
U. Clancy, C. Arteaga-Reyes, D. Jaime Garcia, M.D.C. Valdés Hernández, M. Stringer, M.J. Thrippleton, F.M. Chappell, A.C.C. Jochems, X. Liu, Y. Cheng, and J. Zhang hold grants from government or charitable agencies that funded the research. O.K.L. Hamilton was supported by the Medical Research Council (MC_UU_00022/2) and the Scottish Chief Scientist Office (SPHSU17) and holds grants from government or charitable agencies that funded the research. F.N. Doubal and J.M. Wardlaw hold grants from government or charitable agencies that funded the research. All other authors report no disclosures. Go to
Figures
References
-
- Goeldlin MB, Vynckier J, Mueller M, et al. . Small vessel disease burden and risk of recurrent cerebrovascular events in patients with lacunar stroke and intracerebral haemorrhage attributable to deep perforator arteriolopathy. Eur Stroke J. 2023;8(4):989-1000. doi:10.1177/23969873231193237 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical