

A Database Tool Integrating Genomic and Pharmacologic Data from Adrenocortical Carcinoma Cell Lines, PDX, and Patient Samples
- PMID: 39162009
- PMCID: PMC11389377
- DOI: 10.1158/2767-9764.CRC-24-0100
A Database Tool Integrating Genomic and Pharmacologic Data from Adrenocortical Carcinoma Cell Lines, PDX, and Patient Samples
Abstract
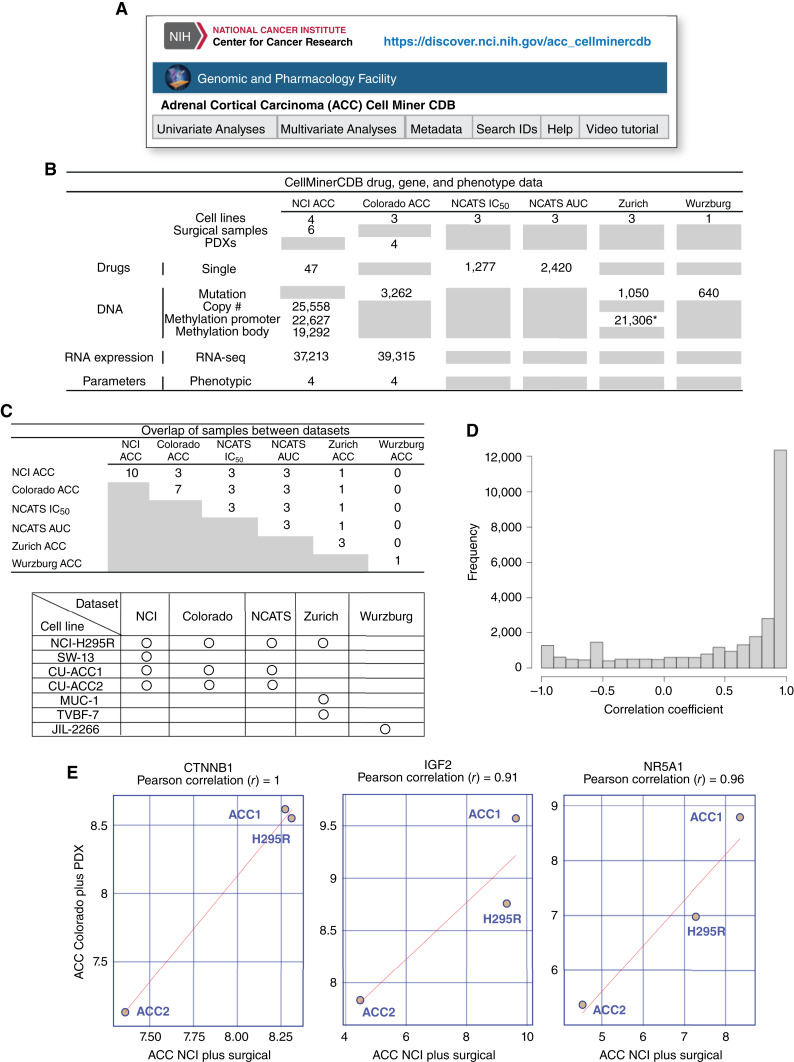
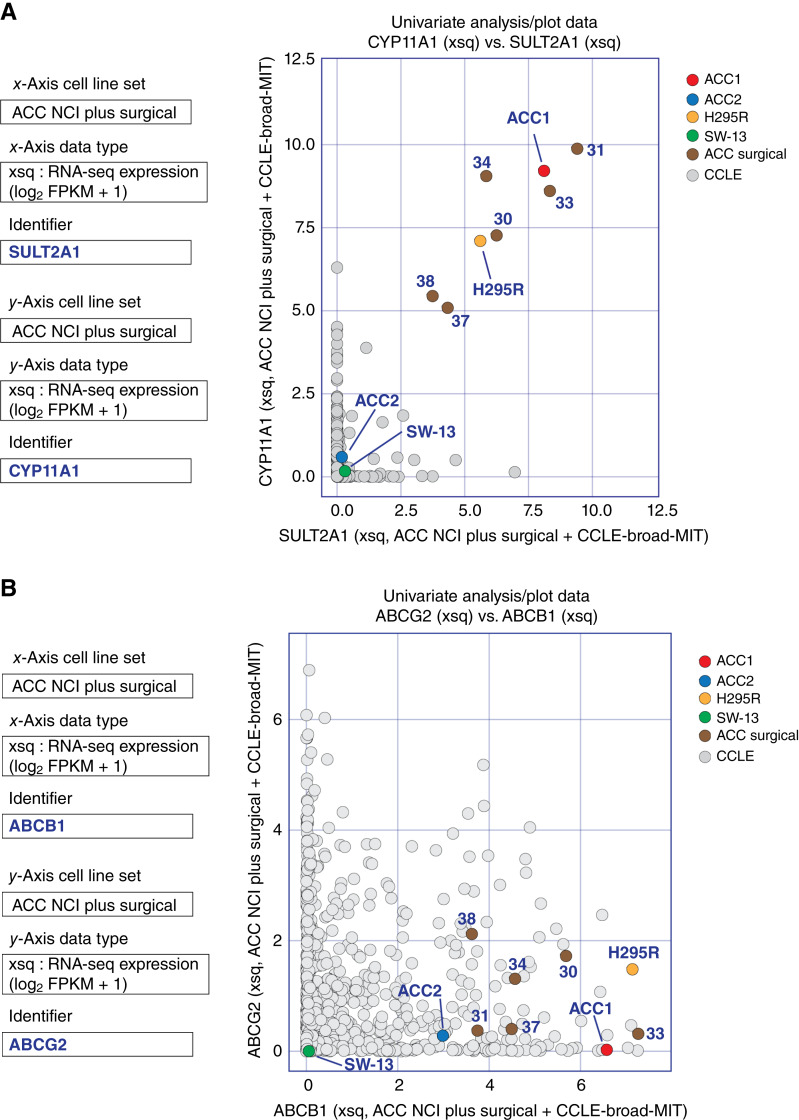
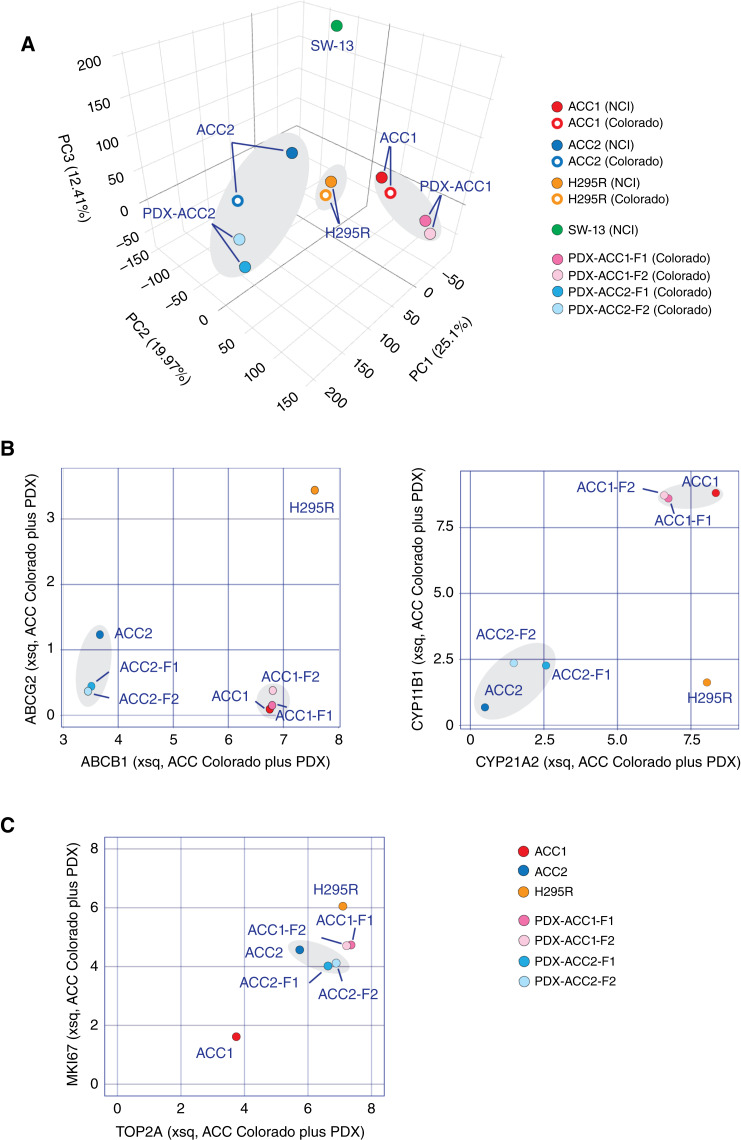
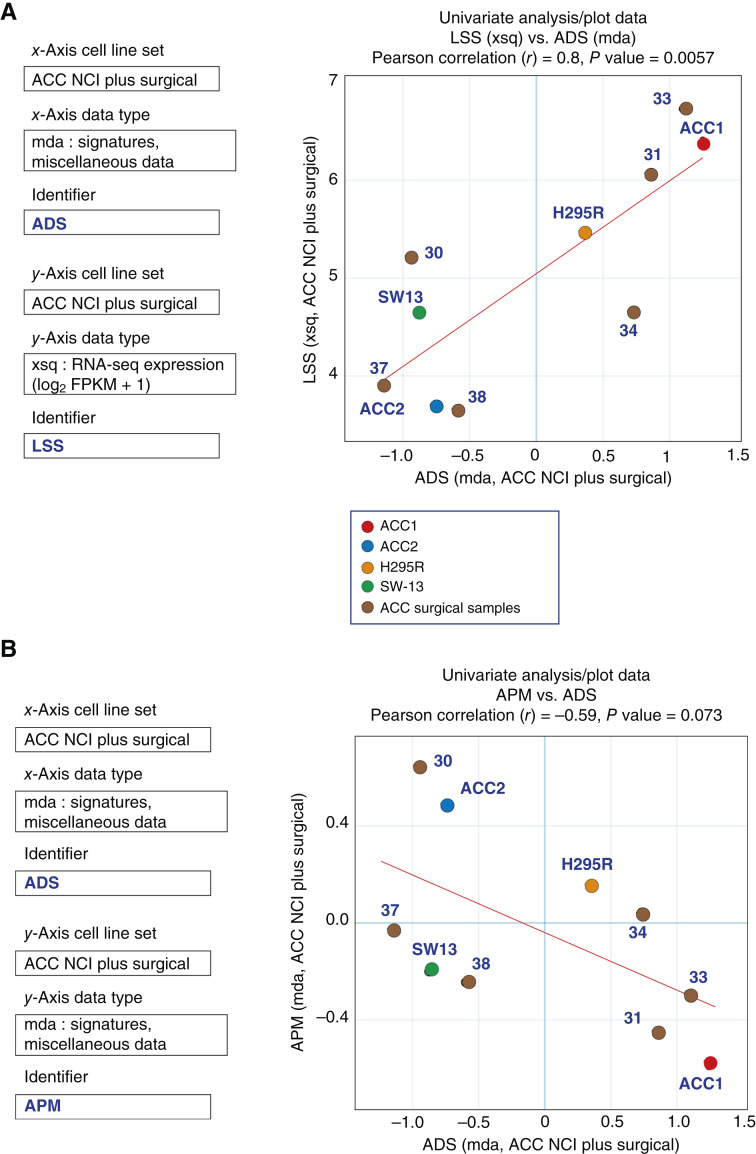
Adrenocortical carcinoma (ACC) is a rare and highly heterogeneous disease with a notably poor prognosis due to significant challenges in diagnosis and treatment. Emphasizing on the importance of precision medicine, there is an increasing need for comprehensive genomic resources alongside well-developed experimental models to devise personalized therapeutic strategies. We present ACC_CellMinerCDB, a substantive genomic and drug sensitivity database (available at https://discover.nci.nih.gov/acc_cellminercdb) comprising ACC cell lines, patient-derived xenografts, surgical samples, and responses to more than 2,400 drugs examined by the NCI and National Center for Advancing Translational Sciences. This database exposes shared genomic pathways among ACC cell lines and surgical samples, thus authenticating the cell lines as research models. It also allows exploration of pertinent treatment markers such as MDR-1, SOAT1, MGMT, MMR, and SLFN11 and introduces the potential to repurpose agents like temozolomide for ACC therapy. ACC_CellMinerCDB provides the foundation for exploring larger preclinical ACC models.
Significance: ACC_CellMinerCDB, a comprehensive database of cell lines, patient-derived xenografts, surgical samples, and drug responses, reveals shared genomic pathways and treatment-relevant markers in ACC. This resource offers insights into potential therapeutic targets and the opportunity to repurpose existing drugs for ACC therapy.
©2024 The Authors; Published by the American Association for Cancer Research.
Conflict of interest statement
Y. Arakawa reports grants from the Japanese Society of Clinical Pharmacology and Therapeutics during the conduct of the study. N. Roper reports grants from the Department of Defense Lung Cancer Career Development Award and grants from ADC Therapeutics during the conduct of the study. W.C. Reinhold reports a patent to E-041-2018-0 pending. K. Kiseljak-Vassiliades reports other from HRA Pharma outside the submitted work. No disclosures were reported by the other authors.
Figures
Similar articles
-
Establishment and characterization of the first pediatric adrenocortical carcinoma xenograft model identifies topotecan as a potential chemotherapeutic agent.Clin Cancer Res. 2013 Apr 1;19(7):1740-7. doi: 10.1158/1078-0432.CCR-12-3354. Epub 2013 Feb 13. Clin Cancer Res. 2013. PMID: 23406775 Free PMC article.
-
Targeted Molecular Analysis in Adrenocortical Carcinomas: A Strategy Toward Improved Personalized Prognostication.J Clin Endocrinol Metab. 2018 Dec 1;103(12):4511-4523. doi: 10.1210/jc.2018-01348. J Clin Endocrinol Metab. 2018. PMID: 30113656
-
Preclinical targeting of the type I insulin-like growth factor receptor in adrenocortical carcinoma.J Clin Endocrinol Metab. 2009 Jan;94(1):204-12. doi: 10.1210/jc.2008-1456. Epub 2008 Oct 14. J Clin Endocrinol Metab. 2009. PMID: 18854392 Free PMC article.
-
Update on in-vivo preclinical research models in adrenocortical carcinoma.Curr Opin Endocrinol Diabetes Obes. 2020 Jun;27(3):170-176. doi: 10.1097/MED.0000000000000543. Curr Opin Endocrinol Diabetes Obes. 2020. PMID: 32304391 Free PMC article. Review.
-
Management of Adrenocortical Carcinoma.Curr Oncol Rep. 2019 Feb 23;21(3):20. doi: 10.1007/s11912-019-0773-7. Curr Oncol Rep. 2019. PMID: 30798468 Review.
References
-
- Balasubramaniam S, Fojo T. Practical considerations in the evaluation and management of adrenocortical cancer. Semin Oncol 2010;37:619–26. - PubMed
-
- Terzolo M, Berruti A. Adjunctive treatment of adrenocortical carcinoma. Curr Opin Endocrinol Diabetes Obes 2008;15:221–6. - PubMed
-
- Fassnacht M, Terzolo M, Allolio B, Baudin E, Haak H, Berruti A, et al. . Combination chemotherapy in advanced adrenocortical carcinoma. N Engl J Med 2012;366:2189–97. - PubMed
-
- Sbiera S, Schmull S, Assie G, Voelker H-U, Kraus L, Beyer M, et al. . High diagnostic and prognostic value of steroidogenic factor-1 expression in adrenal tumors. J Clin Endocrinol Metab 2010;95:E161–71. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
