

Management of Moderate-to-Severe Atopic Dermatitis in Adults: A Cross-Sectional Survey of Dermatologists Within the Asia-Pacific Region
- PMID: 39162764
- PMCID: PMC11393370
- DOI: 10.1007/s13555-024-01246-5
Management of Moderate-to-Severe Atopic Dermatitis in Adults: A Cross-Sectional Survey of Dermatologists Within the Asia-Pacific Region
Abstract
Introduction: Limited evidence is available on real-world management of atopic dermatitis (AD) among Asian adults. This cross-sectional study aimed to assess current approaches in AD diagnosis and management in Asia.
Methods: Practising dermatologists regularly treating patients with moderate-to-severe AD were recruited from eight Asia-Pacific territories, namely Mainland China, Hong Kong, India, Japan, Singapore, South Korea, Taiwan, and Thailand. A survey was administered to eligible dermatologists after screening and taking informed consent. Data from fully completed submissions were analysed using descriptive statistics. The study was reviewed by the institutional review board in each territory.
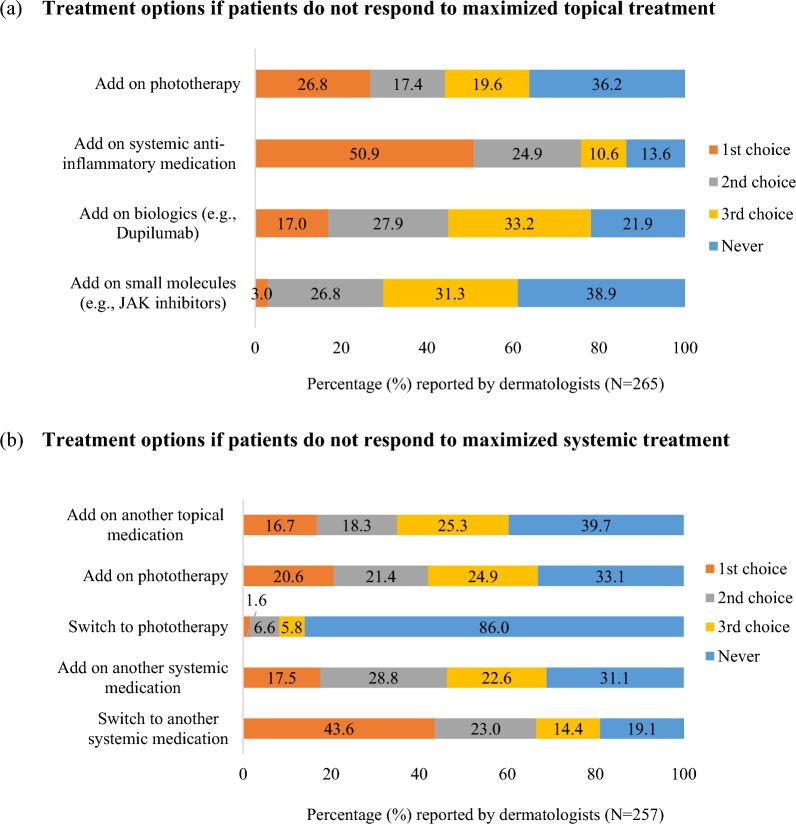
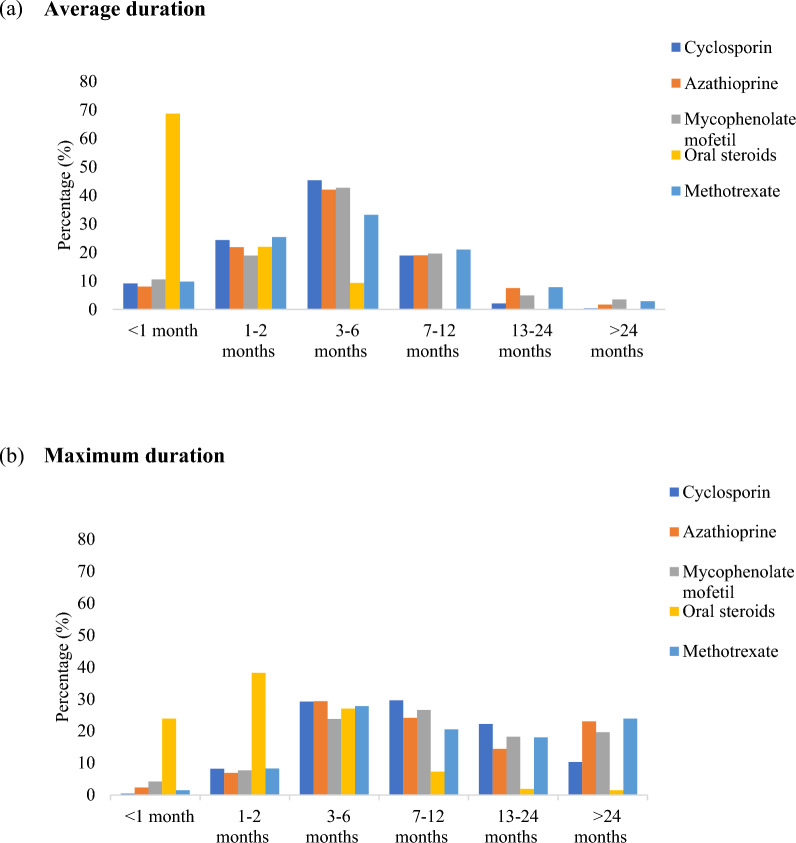
Results: Data from 271 dermatologists were included for analysis. About one-third (31.7%) reported that they referred to the Hanifin and Rajka criteria during diagnosis. The majority of dermatologists used clinical impression when assessing AD severity and treatment response. Reduction of eczema and pruritus was the primary treatment objective when managing both acute (98.1%) and chronic (69.1%) AD. More than half of dermatologists preferred adding systemic anti-inflammatory medication for patients who did not respond to maximized topical treatment, while 43.6% would switch to another systemic medication for those failing to respond to maximized systemic treatment. Topical corticosteroids were frequently selected by dermatologists. For systemic therapies, oral corticosteroids were most frequently used, followed by cyclosporin and dupilumab. Narrow-band ultraviolet B was the most common phototherapy reported (84.9%). There was considerable variation in estimated average and maximum durations of therapies used to treat AD.
Conclusion: This study has provided insights on the real-world management of moderate-to-severe AD in the Asia-Pacific region. The diverse approaches in diagnosis and treatment highlight the multifactorial nature of AD, reliance on clinical judgement, and importance of personalized care. To improve outcomes in patients with AD, it will be crucial to develop biomarkers for diagnosis, reduce subjectivity in assessment, as well as promote access to newer and effective therapies.
Keywords: Asia; Atopic dermatitis; Cross-sectional; Dermatologist; Eczema; Management; Questionnaire; Real-world; Survey; Treatment.
© 2024. The Author(s).
Conflict of interest statement
Han-Fang Liao and Sean Gardiner are employees of Pfizer. Yoko Kataoka has received lecturer honoraria from Sanofi, AbbVie, Pfizer and Maruho, and research funding from Sanofi, Leo Pharma, Pfizer, Maruho, Lilly, AbbVie, Otsuka, Taiho and Amgen. Yung Chan is a speaker for AbbVie, Bioderma, Galderma, Inova, Eli Lily, Lumenis, Menarini and Pfizer; an advisory board member for AbbVie, Bayer, Bioderma, CeraVe, Eli Lilly, Menarini, Pfizer, Sanofi, Quanta System and Janssen. Chia-Yu Chu is an investigator for AbbVie, Amgen, Dermira, Eli Lilly, Janssen, Novartis, Oneness Biotech, Pfizer, Regeneron Pharmaceuticals Inc., Roche and Sanofi; a consultant for AbbVie, Amgen, Eli Lilly, GlaxoSmithKline, Janssen, Novartis, Pfizer, Roche and Sanofi; a speaker for AbbVie, Eli Lilly, GlaxoSmithKline, Janssen, Mylan, Novartis, Pfizer, Roche, Sanofi and Viatris; and an advisory board member for AbbVie, Amgen, Mylan, Pfizer, Roche, Sanofi and Viatris. Nisha Suyien Chandran has received fees for participation in advisory boards from AbbVie, Johnson & Johnson, Sanofi, Pfizer, DKSH, L’Oreal and Novartis; investigator fees for clinical trials from AbbVie, Novartis, Amgen, Sanofi and Boehringer Ingelheim; and speaker honoraria from Galderma, Johnson & Johnson, LEO, Pfizer, Sanofi and Lion Corporation. All other authors have no conflict of interest.
Figures




References
-
- Langan SM, Irvine AD, Weidinger S. Atopic dermatitis. Lancet. 2020;396(10247):345–60. - PubMed
-
- Williams H, Stewart A, von Mutius E, Cookson W, Anderson HR, International Study of Asthma and Allergies in Childhood (ISAAC) Phase One and Three Study Groups. Is eczema really on the increase worldwide? J Allergy Clin Immunol. 2008;121(4):947-54.e15. - PubMed
-
- Yong AM-Y, Tay Y-K. Atopic dermatitis: racial and ethnic differences. Dermatol Clin. 2017;35(3):395–402. - PubMed
-
- Carroll CL, Balkrishnan R, Feldman SR, Fleischer AB Jr, Manuel JC. The burden of atopic dermatitis: impact on the patient, family, and society. Pediatr Dermatol. 2005;22(3):192–9. - PubMed
LinkOut - more resources
Full Text Sources
