

Conservative or liberal oxygen targets in patients on venoarterial extracorporeal membrane oxygenation
- PMID: 39162827
- PMCID: PMC11377512
- DOI: 10.1007/s00134-024-07564-8
Conservative or liberal oxygen targets in patients on venoarterial extracorporeal membrane oxygenation
Erratum in
-
Correction: Conservative or liberal oxygen targets in patients on venoarterial extracorporeal membrane oxygenation.Intensive Care Med. 2024 Dec;50(12):2241-2242. doi: 10.1007/s00134-024-07677-0. Intensive Care Med. 2024. PMID: 39412548 Free PMC article. No abstract available.
Abstract
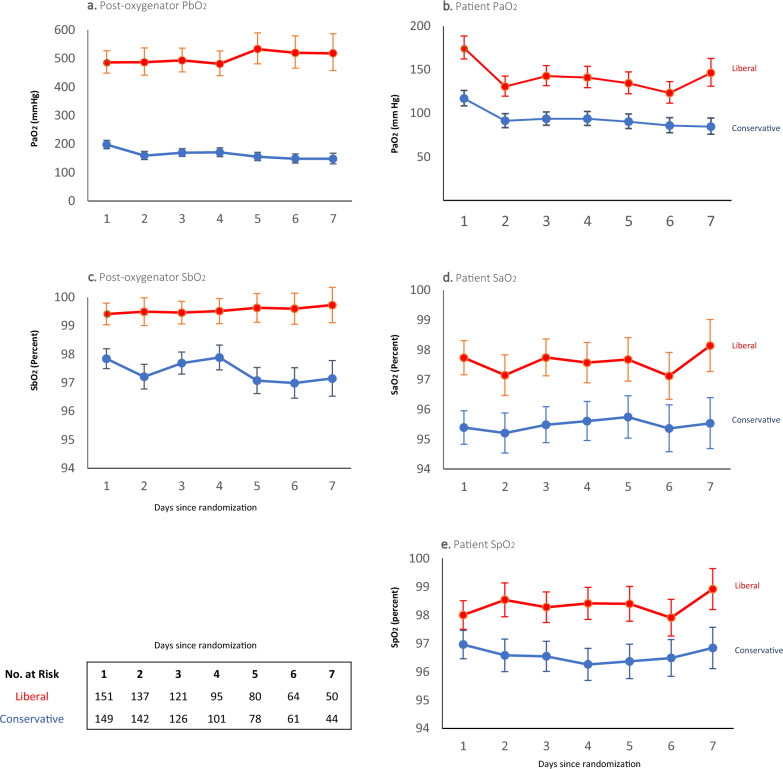
Purpose: Patients receiving venoarterial extracorporeal membrane oxygenation (VA-ECMO) frequently develop arterial hyperoxaemia, which may be harmful. However, lower oxygen saturation targets may also lead to harmful episodes of hypoxaemia.
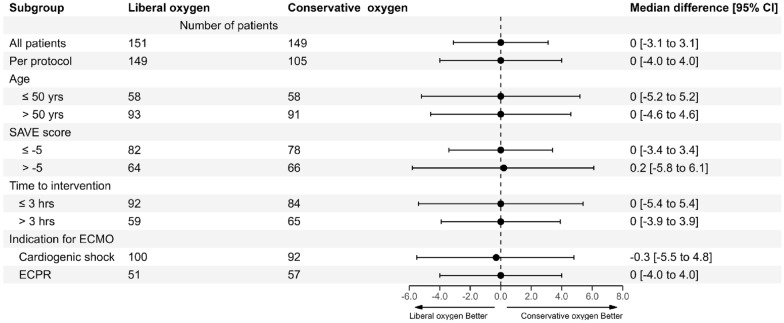
Methods: In this registry-embedded, multicentre trial, we randomly assigned adult patients receiving VA-ECMO in an intensive care unit (ICU) to either a conservative (target SaO2 92-96%) or to a liberal oxygen strategy (target SaO2 97-100%) through controlled oxygen administration via the ventilator and ECMO gas blender. The primary outcome was the number of ICU-free days to day 28. Secondary outcomes included ICU-free days to day 60, mortality, ECMO and ventilation duration, ICU and hospital lengths of stay, and functional outcomes at 6 months.
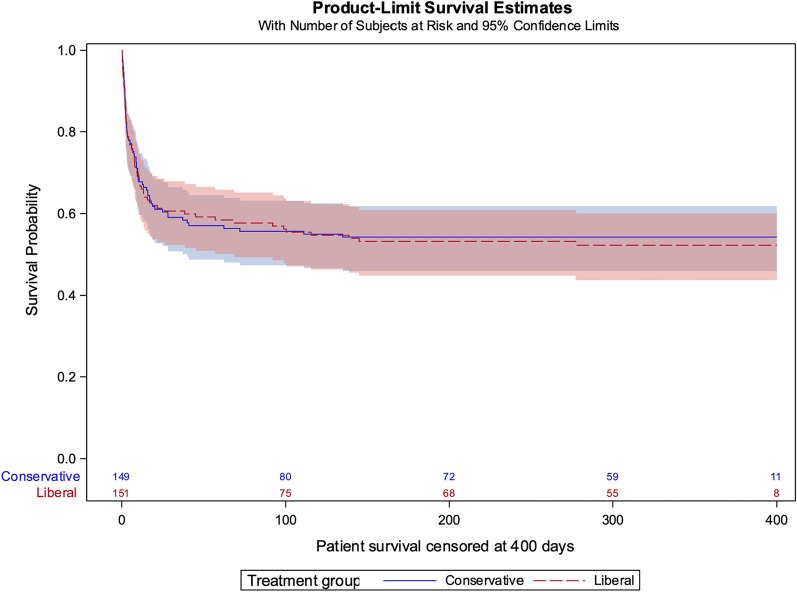
Results: From September 2019 through June 2023, 934 patients who received VA-ECMO were reported to the EXCEL registry, of whom 300 (192 cardiogenic shock, 108 refractory cardiac arrest) were recruited. We randomised 149 to a conservative and 151 to a liberal oxygen strategy. The median number of ICU-free days to day 28 was similar in both groups (conservative: 0 days [interquartile range (IQR) 0-13.7] versus liberal: 0 days [IQR 0-13.7], median treatment effect: 0 days [95% confidence interval (CI) - 3.1 to 3.1]). Mortality at day 28 (59/159 [39.6%] vs 59/151 [39.1%]) and at day 60 (64/149 [43%] vs 62/151 [41.1%] were similar in conservative and liberal groups, as were all other secondary outcomes and adverse events. The conservative group experienced 44 (29.5%) major protocol deviations compared to 2 (1.3%) in the liberal oxygen group (P < 0.001).
Conclusions: In adults receiving VA-ECMO in ICU, a conservative compared to a liberal oxygen strategy, did not affect the number of ICU-free days to day 28.
Keywords: ECMO; Extracorporeal membrane oxygenation; Hyperoxaemia; Hyperoxia; Oxygen target.
© 2024. The Author(s).
Conflict of interest statement
The corresponding author (David Pilcher) states on behalf of all authors, that there are no conflicts of interest to declare.
Figures
References
-
- Lorusso R, Shekar K, MacLaren G, Schmidt M, Pellegrino V, Meyns B, Haft J, Vercaemst L, Pappalardo F, Bermudez C, Belohlavek J, Hou X, Boeken U, Castillo R, Donker DW, Abrams D, Ranucci M, Hryniewicz K, Chavez I, Chen YS, Salazar L, Whitman G (2021) ELSO interim guidelines for venoarterial extracorporeal membrane oxygenation in adult cardiac patients. ASAIO J 67:827–844 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
