

Co-morbid sarcopenia and low bone mineral density in young paediatric cancer survivors
- PMID: 39164071
- PMCID: PMC11446677
- DOI: 10.1002/jcsm.13563
Co-morbid sarcopenia and low bone mineral density in young paediatric cancer survivors
Abstract
Background: Sarcopenia and low areal bone mineral density (aBMD) are prevalent musculoskeletal complications after paediatric cancer treatment. However, their relationship has not been examined in young paediatric cancers survivors. This study aimed to evaluate aBMD differences according to sarcopenia status and the risk of low aBMD Z-score in young paediatric cancer survivors with sarcopenia confirmed/probable.
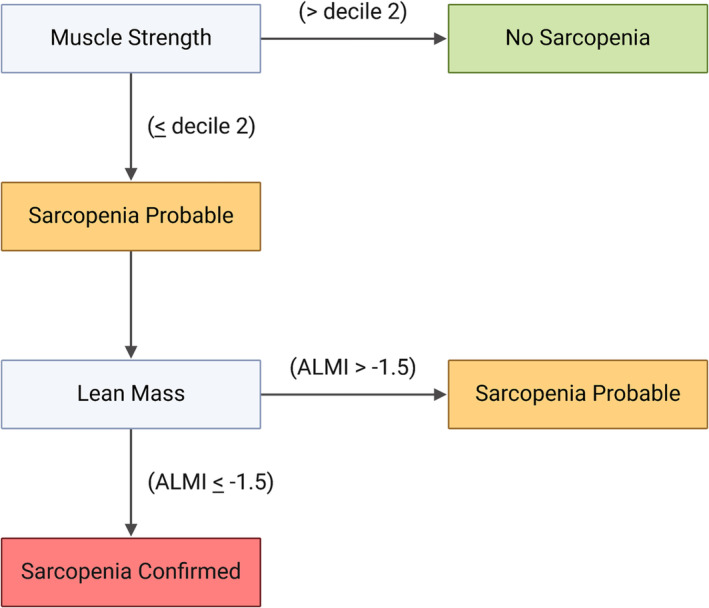
Methods: This cross-sectional study included 116 paediatric cancer survivors (12.1 ± 3.3 years old; 42.2% female). Handgrip strength was used to assessed muscle strength. Dual-energy X-ray absorptiometry estimated aBMD (g/cm2) and appendicular lean mass index (ALMI, kg/m2). 'No sarcopenia' was defined when muscle strength was >decile 2. 'Sarcopenia probable' was defined when muscle strength was ≤ decile 2 and ALMI Z-score was > -1.5 standard deviation (SD). 'Sarcopenia confirmed' was defined when muscle strength was ≤ decile 2 and ALMI Z-score ≤ -1.5 SD. Analysis of covariance and logistic regression, adjusted for time from treatment completion, radiotherapy exposure, calcium intake, and physical activity, was used to evaluate aBMD and estimate the odds ratios (ORs) of low aBMD (aBMD Z-score < -1.0).
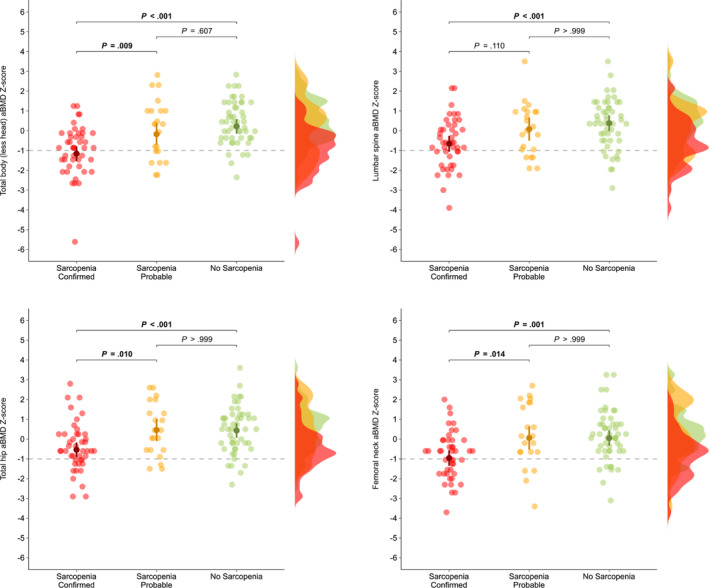
Results: Survivors with sarcopenia confirmed had significantly lower aBMD than those without sarcopenia at total body (-1.2 [95% CI: -1.5 to -0.8] vs. 0.2 [-0.2 to 0.6], P < 0.001), lumbar spine (-0.7 [-1.1 to -0.3] vs. 0.4 [0.0 to 0.8], P < 0.001), total hip (-0.5 [-0.9 to -0.2] vs. 0.4 [0.1 to 0.8], P < 0.001), and femoral neck (-1.0 [-1.4 to -0.6] vs. 0.1 [-0.3 to 0.4], P = 0.001). Compared with survivors with sarcopenia probable, survivors with sarcopenia confirmed had significantly lower aBMD Z-score at total body (-1.2 [-1.5 to -0.8] vs. -0.2 [-0.7 to 0.4], P = 0.009), total hip (-0.5 [-0.9 to -0.2] vs. 0.5 [-0.1 to 1.0], P = 0.010), and femoral neck (-1.0 [-1.4 to -0.6] vs. 0.1 [-0.5 to 0.7], P = 0.014). Survivors with sarcopenia confirmed were at higher risk of low aBMD Z-score at the total body (OR: 6.91, 95% CI: 2.31-24.15), total hip (OR: 2.98, 1.02-9.54), and femoral neck (OR: 4.72, 1.72-14.19), than those without sarcopenia. Survivors with sarcopenia probable were at higher risk of low aBMD Z-score at the total body (OR: 4.13, 1.04-17.60) than those without sarcopenia.
Conclusions: Young paediatric cancer survivors with sarcopenia present higher risk of low aBMD. Resistance training-based interventions designed to mitigate osteosarcopenia in this population should be implemented at early stages.
Keywords: Bone health; Cachexia; Childhood cancer; Exercise; Muscular health.
© 2024 The Author(s). Journal of Cachexia, Sarcopenia and Muscle published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare that they do not have competing interests.
Figures
References
-
- Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin 2024;74:12–49. - PubMed
-
- Marcucci G, Beltrami G, Tamburini A, Body JJ, Confavreux CB, Hadji P, et al. Bone health in childhood cancer: review of the literature and recommendations for the management of bone health in childhood cancer survivors. Ann Oncol 2019;30:908–920. - PubMed
-
- Chemaitilly W, Cohen LE, Mostoufi‐Moab S, Patterson BC, Simmons JH, Meacham LR, et al. Endocrine late effects in childhood cancer survivors. J Clin Oncol 2018;36:2153–2159. - PubMed
-
- van Santen HM, Chemaitilly W, Meacham LR, Tonorezos ES, Mostoufi‐Moab S. Endocrine health in childhood cancer survivors. Pediatr Clin North Am 2020;67:1171–1186. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
