

Long-term surveillance study of rituximab originator treated patients with granulomatosis with polyangiitis (GPA) or microscopic polyangiitis (MPA)
- PMID: 39165399
- PMCID: PMC11333760
- DOI: 10.1093/rap/rkae090
Long-term surveillance study of rituximab originator treated patients with granulomatosis with polyangiitis (GPA) or microscopic polyangiitis (MPA)
Abstract
Objectives: Rituximab is used for remission induction and the prevention of relapse in anti-neutrophil cytoplasmic antibody-associated vasculitis (AAV). This study evaluated the incidence of safety events and compared time to first serious adverse event (SAE) between a rituximab cohort and a cohort treated with non-rituximab therapies in a real-life setting.
Methods: Rituximab surveillance study in vasculitis was a retrospective observational study of patients with AAV who received rituximab (MabThera) or other treatments between 2003 and 2017 at a specialist vasculitis clinic. The primary endpoint was time to first SAE.
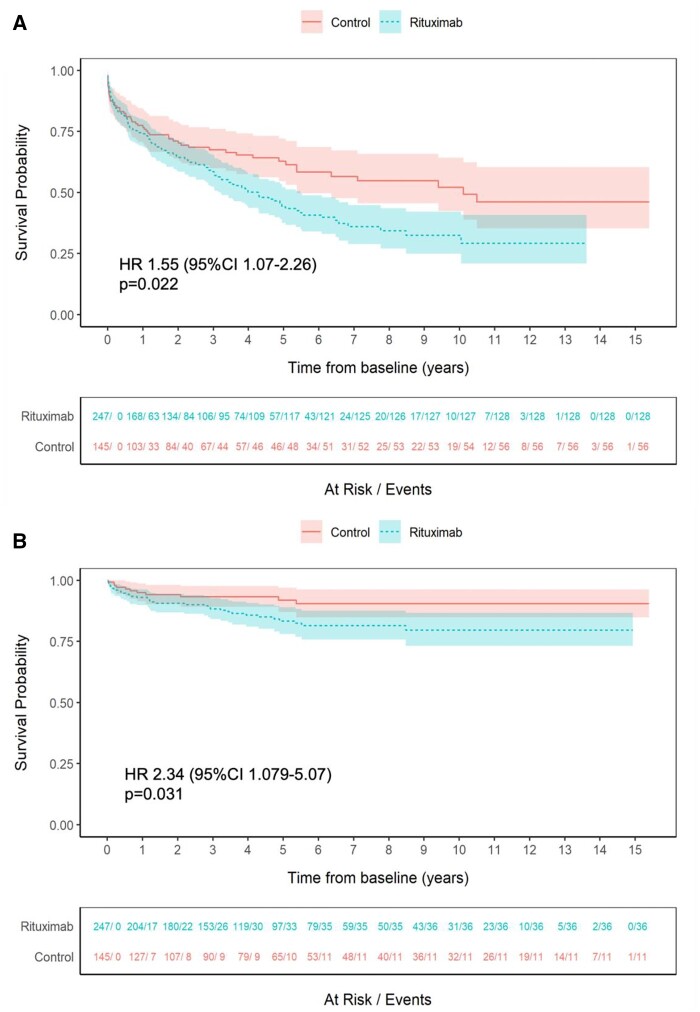
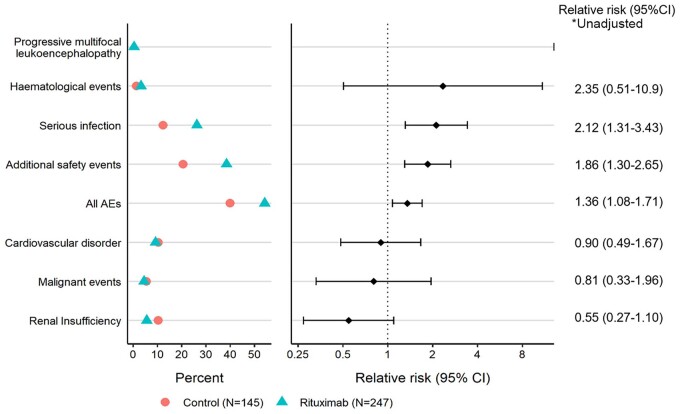
Results: 392 patients were enrolled: 247 in the rituximab and 145 in the control cohorts with a total follow up of 2217 person-years (mean study duration 5.7 years). Mean age was 61 years, 77% had granulomatosis with polyangiitis (GPA). There were differences in baseline characteristics (disease duration and prior immunosuppressive use) between groups. 134/247 patients (54%) in the rituximab and 58/145 (40%) of controls experienced at least one SAE. Time to first SAE was shorter in the rituximab group (hazard ratio (HR) 1.55, 95% CI 1.07-2.26, P = 0.022). Predictors of first SAE were higher vasculitis damage index and the presence of chronic pulmonary or kidney disease. The risk of serious infection was higher in the rituximab group (relative risk (RR) 2.12, 95% CI 1.31-3.43).
Conclusion: Over 40% of patients with AAV experienced at least one SAE. Although shorter time to first SAE and higher risk of infection were observed in the rituximab group, baseline imbalances necessitate a careful interpretation of these results.
Keywords: ANCA-associated vasculitis; rituximab; safety.
© The Author(s) 2024. Published by Oxford University Press on behalf of the British Society for Rheumatology.
Figures
References
-
- Kitching AR, Anders H-J, Basu N. et al. ANCA-associated vasculitis. Nat Rev Dis Primers 2020;6:71. - PubMed
-
- Hoffman GS, Kerr GS, Leavitt RY. et al. Wegener granulomatosis: an analysis of 158 patients. Ann Intern Med 1992;116:488–98. - PubMed
-
- Smith KGC, Jones RB, Burns SM, Jayne DRW.. Long-term comparison of rituximab treatment for refractory systemic lupus erythematosus and vasculitis: remission, relapse, and re-treatment. Arthritis Rheum 2006;54:2970–82. - PubMed
LinkOut - more resources
Full Text Sources