

Comparison of Mixed Reality-Assisted Spinal Puncture with Landmark-Guided Spinal Puncture by Novice Practitioners: A Pilot Study
- PMID: 39165722
- PMCID: PMC11334921
- DOI: 10.2147/JPR.S470285
Comparison of Mixed Reality-Assisted Spinal Puncture with Landmark-Guided Spinal Puncture by Novice Practitioners: A Pilot Study
Abstract
Background: Performing spinal anaesthesia in elderly patients with ligament calcification or hyperostosis is challenging for novice practitioners. This pilot study aimed to compare the effectiveness of mixed reality-assisted spinal puncture (MRasp) with that of landmark-guided spinal puncture (LGsp) by novice practitioners in elderly patients.
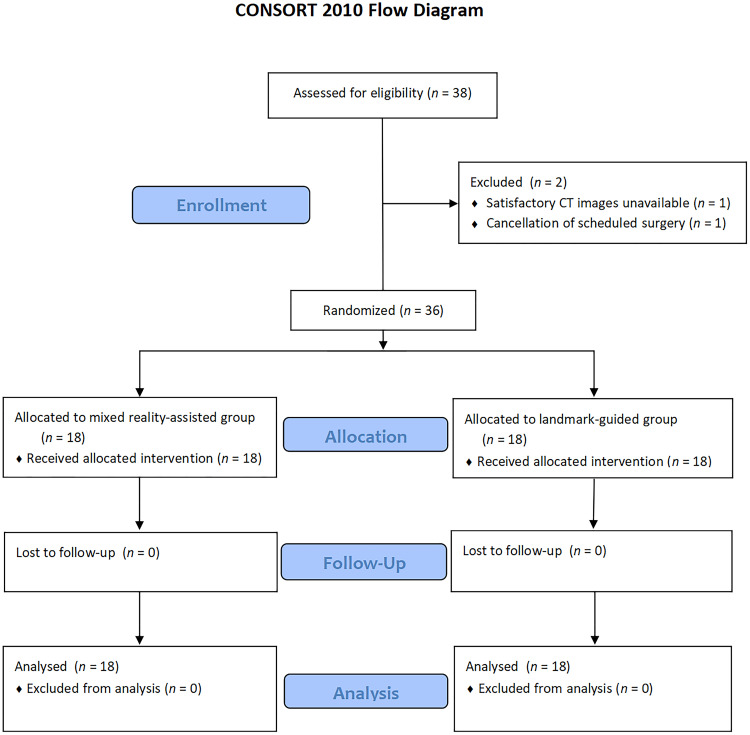
Methods: In this pilot study, 36 patients (aged ≥65 years) scheduled for elective surgery under spinal anaesthesia by anaesthesiology residents were included. Patients were randomly assigned to the MRasp group (n = 18) or the LGsp group (n = 18). The outcomes included the number of needle insertion attempts, redirection attempts, passes, the rate of successful first-attempt needle insertion, the rate of successful first needle pass, the spinal puncture time, the total procedure time, and the incidence of perioperative complications.
Results: The median number of needle insertion attempts was significantly fewer in the MRasp group than in the LGsp group (1.0 vs 2.0, P = 0.023). The proportion of patients with successful first-attempt needle insertion was 72.2% in the MRasp group and 44.4% in the LGsp group (P = 0.176). The incidence of perioperative complications did not significantly differ between the two groups.
Conclusion: This pilot study found that novice practitioners made significantly fewer needle insertion attempts in the MRasp group compared to the LGsp group when performing spinal anaesthesia on elderly patients. A future randomized controlled trial (RCT) is warranted to validate its effectiveness.
Trial registration: This trial was registered at https://www.chictr.org.cn/showproj.html?proj=178960 (ChiCTR-IPR-2300068520). Public title: Mixed reality-assisted versus landmark-guided spinal puncture in elderly patients: a randomized controlled pilot study. Principal investigator: Lei Gao. The registration date was February 22, 2023. The date of the first participant enrolment was February 27, 2023.
Keywords: augmented reality; computer simulation; mixed reality; spinal puncture.
Plain language summary
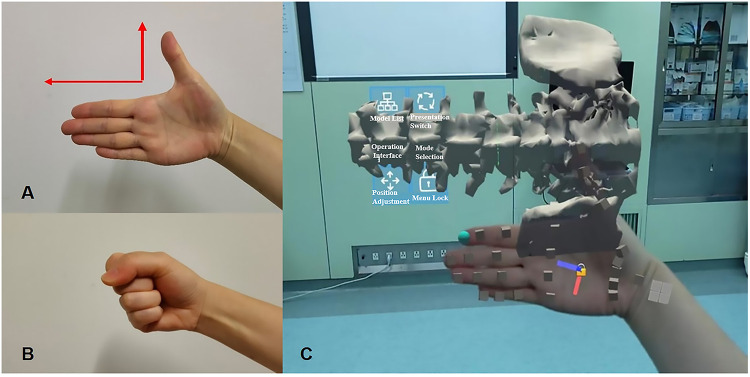
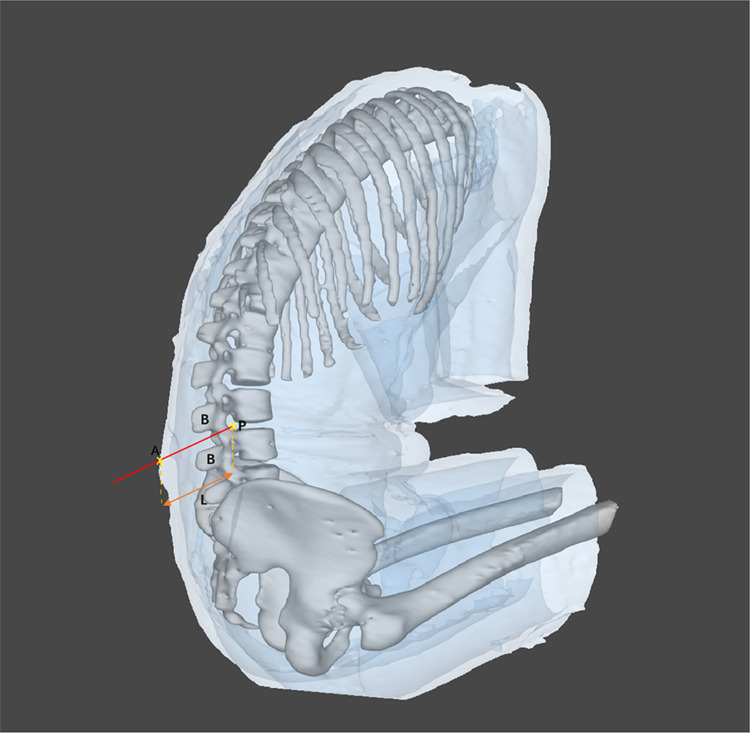
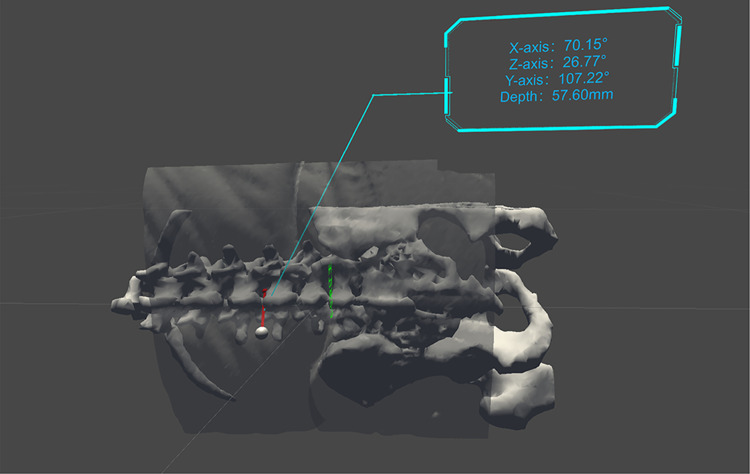
We developed virtual spine-presenting technology and patented optimal trajectory design technology to assist in spinal puncture and reported that the median number of needle insertion attempts was significantly fewer in the mixed reality-assisted spinal puncture group than in the landmark-guided spinal puncture group.
© 2024 Gao et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest in this work.
Figures

Similar articles
-
Mixed reality-assisted versus landmark-guided spinal puncture in elderly patients: protocol for a stratified randomized controlled trial.Trials. 2024 Nov 19;25(1):780. doi: 10.1186/s13063-024-08628-2. Trials. 2024. PMID: 39558217 Free PMC article.
-
Landmark-guided versus modified ultrasound-assisted Paramedian techniques in combined spinal-epidural anesthesia for elderly patients with hip fractures: a randomized controlled trial.BMC Anesthesiol. 2020 Sep 28;20(1):248. doi: 10.1186/s12871-020-01172-x. BMC Anesthesiol. 2020. PMID: 32988366 Free PMC article. Clinical Trial.
-
[Ultrasound imaging increases first-attempt success rate of neuraxial block in elderly patients].Zhonghua Yi Xue Za Zhi. 2016 Nov 22;96(43):3459-3463. doi: 10.3760/cma.j.issn.0376-2491.2016.43.004. Zhonghua Yi Xue Za Zhi. 2016. PMID: 27903338 Chinese.
-
Ultrasound-Assisted Technology Versus the Conventional Landmark Location Method in Spinal Anesthesia for Cesarean Delivery in Obese Parturients: A Randomized Controlled Trial.Anesth Analg. 2019 Jul;129(1):155-161. doi: 10.1213/ANE.0000000000003795. Anesth Analg. 2019. PMID: 30234528 Clinical Trial.
-
Conventional landmark palpation versus preprocedural ultrasound for neuraxial procedures in nonobstetric patients: A systematic review with meta-analysis and trial sequential analysis of randomised controlled trials.Eur J Anaesthesiol. 2021 Aug 1;38(Suppl 2):S73-S86. doi: 10.1097/EJA.0000000000001525. Eur J Anaesthesiol. 2021. PMID: 33883460
Cited by
-
Mixed reality-assisted versus landmark-guided spinal puncture in elderly patients: protocol for a stratified randomized controlled trial.Trials. 2024 Nov 19;25(1):780. doi: 10.1186/s13063-024-08628-2. Trials. 2024. PMID: 39558217 Free PMC article.
-
Enhancing endoscopic spine surgery with intraoperative augmented reality: A case report.Int J Surg Case Rep. 2025 Jun;131:111342. doi: 10.1016/j.ijscr.2025.111342. Epub 2025 Apr 23. Int J Surg Case Rep. 2025. PMID: 40279997 Free PMC article.
-
An attempt to evaluate the use of mixed reality in surgically treated pediatric oncology patients.NPJ Digit Med. 2025 May 9;8(1):262. doi: 10.1038/s41746-025-01638-7. NPJ Digit Med. 2025. PMID: 40346298 Free PMC article.
References
LinkOut - more resources
Full Text Sources
