

Outcomes From Mechanical Thrombectomy for Deep Vein Thrombosis: Insights From the PINC AI Healthcare Database
- PMID: 39166156
- PMCID: PMC11330914
- DOI: 10.1016/j.jscai.2024.102149
Outcomes From Mechanical Thrombectomy for Deep Vein Thrombosis: Insights From the PINC AI Healthcare Database
Abstract
Background: Mechanical thrombectomy (MT) is playing an increasingly important role in treating deep vein thrombosis (DVT). Although degrees of safety and efficacy have been shown in independent studies, there remains a lack of comparative evidence between MT devices. To address this, we aimed to compare demographics, clinical outcomes, and resource metrics of patients receiving MT for DVT with 3 common devices using a real-world database.
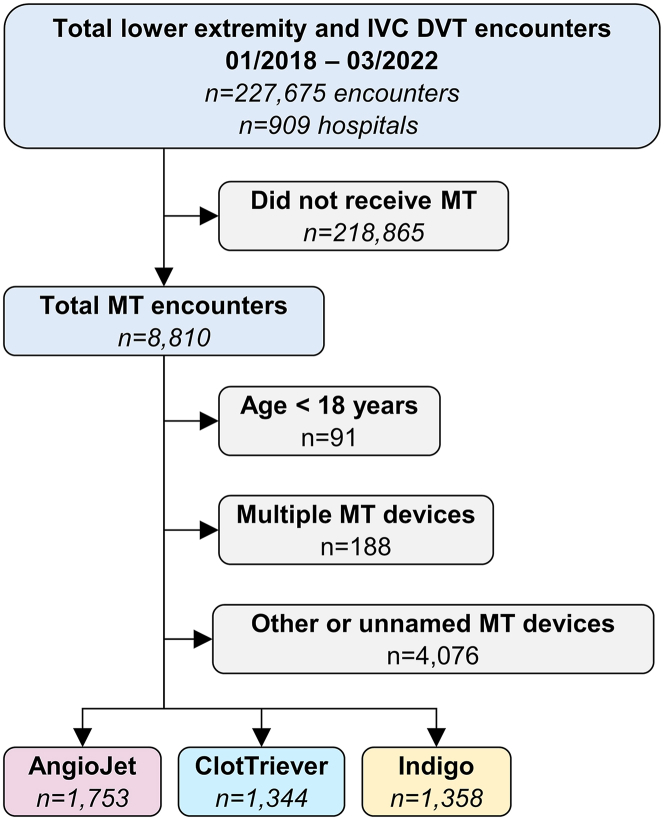
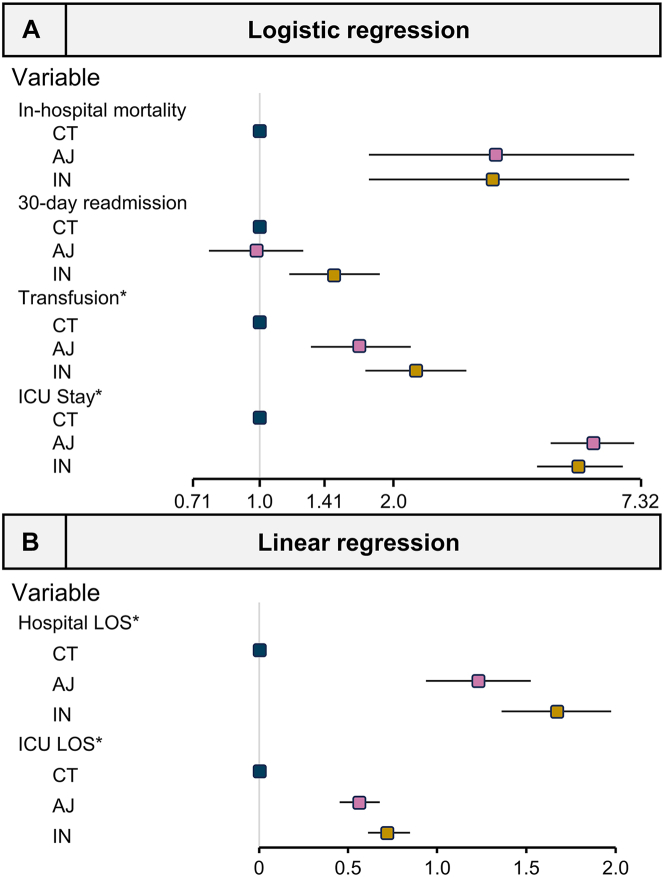
Methods: Patients receiving MT for DVT between January 2018 and March 2022 were identified from the PINC AI Healthcare Database and divided into analysis populations for the AngioJet ZelanteDVT (AJ), the ClotTriever system (CT), and the Indigo system (IN). Rates of in-hospital mortality, resource utilization, and 30-day readmission were compared. Regression modeling was performed to adjust for potential covariates and compare outcomes.
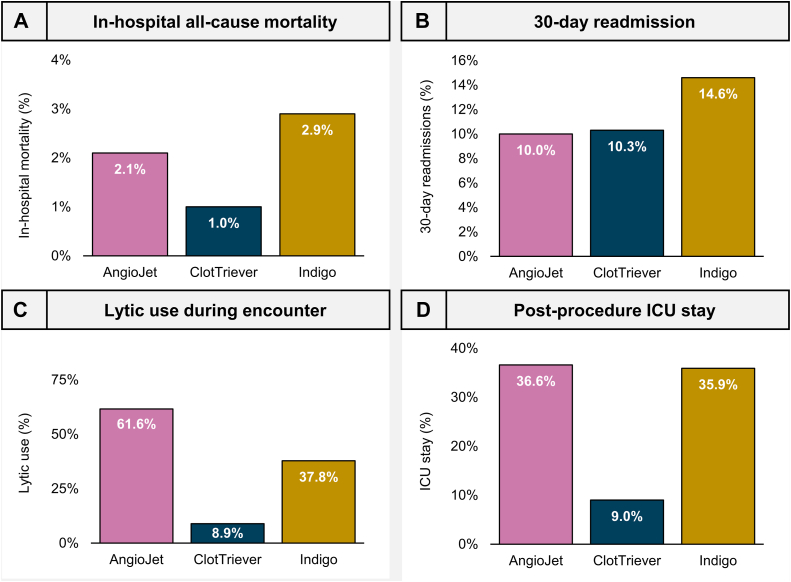
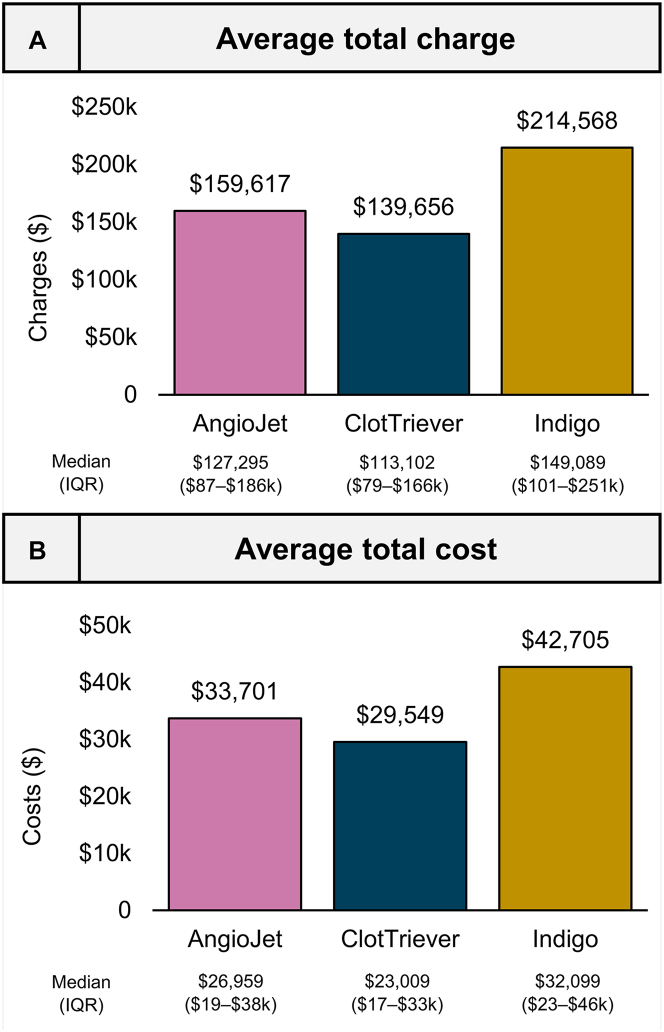
Results: A total of 4455 MT encounters were identified and met inclusion criteria (AJ, 1753; CT, 1344; IN, 1358). In-hospital mortality ranged from 1.0% (CT) to 2.9% (IN), with modeling predicting significantly higher odds for the AJ (odds ratio [OR], 3.42) and IN (OR, 3.38) groups. Similarly, higher rates of resource utilization were predicted in the AJ and IN groups when compared with the reference group (CT). Average costs ranged from $29,549 (CT: SD, $30,705) to $42,705 (IN: SD, $41,114). Thirty-day readmissions ranged from 10.0% (AJ) to 14.6% (IN), while modeling predicted significantly greater odds for the IN group (OR, 1.47).
Conclusions: These results suggest that all MT interventions may be unequal in terms of outcomes and resources, with the CT device associated with lower in-hospital mortality and resource burden.
Keywords: deep vein thrombosis; intervention; lower extremity; real-world data; venous thrombosis.
© 2024 The Author(s).
Conflict of interest statement
Derek Mittleider is a consultant for Boston Scientific and Inari Medical. C. Michael Gibson received research grant support from Inari Medical, Boston Scientific, and Penumbra and consultant for Inari Medical. David Dexter is a consultant for AngioDynamics, Boston Scientific, Penumbra, and Inari Medical.
Figures
References
-
- Baekgaard N. Incidence and location of deep vein thrombosis in the lower extremities: what do we know. Phlebolymphology. 2017;24:97–104.
-
- Kahn S.R., Shrier I., Julian J.A., et al. Determinants and time course of the postthrombotic syndrome after acute deep venous thrombosis. Ann Intern Med. 2008;149(10):698–707. - PubMed
-
- Dexter D.J., Kado H., Schor J., et al. Interim outcomes of mechanical thrombectomy for deep vein thrombosis from the All-Comer CLOUT Registry. J Vasc Surg Venous Lymphat Disord. 2022;10(4):832–840.e2. - PubMed
-
- Maldonado T.S., Dexter D.J., Kado H., et al. Outcomes from the ClotTriever Outcomes Registry show symptom duration may underestimate deep vein thrombus chronicity. J Vasc Surg Venous Lymphat Disord. 2022;10(6):1251–1259. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
