

Tyrosine Kinase 2 Inhibition With Zasocitinib (TAK-279) in Psoriasis: A Randomized Clinical Trial
- PMID: 39167366
- PMCID: PMC11339701
- DOI: 10.1001/jamadermatol.2024.2701
Tyrosine Kinase 2 Inhibition With Zasocitinib (TAK-279) in Psoriasis: A Randomized Clinical Trial
Abstract
Importance: New, effective, and well-tolerated oral therapies are needed for treating psoriasis. Zasocitinib, a highly selective allosteric tyrosine kinase 2 (TYK2) inhibitor, is a potential new oral treatment for this disease.
Objective: To assess the efficacy, safety, and tolerability of zasocitinib in patients with moderate to severe plaque psoriasis.
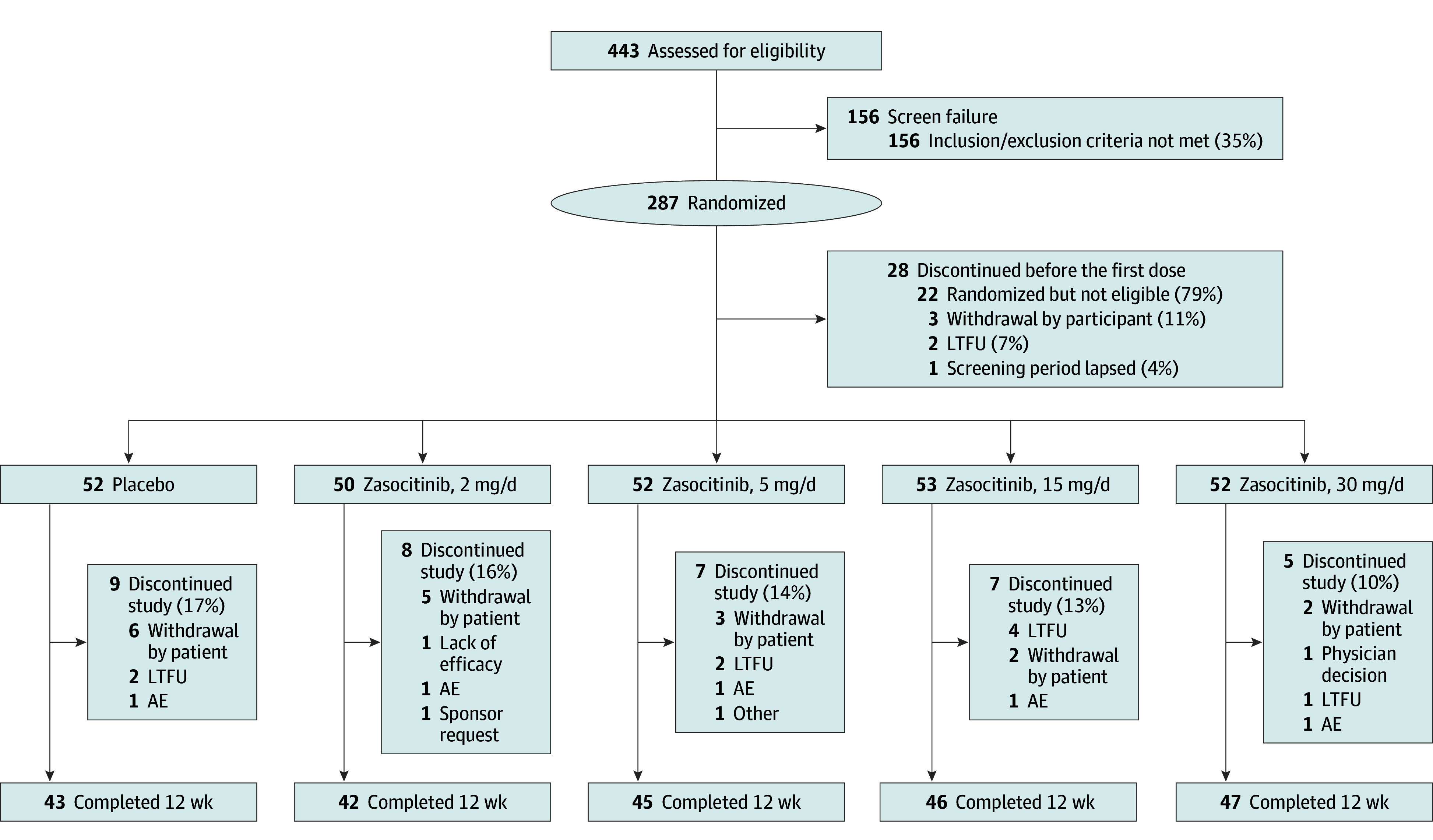
Design, setting, and participants: This phase 2b, randomized, double-blind, placebo-controlled, multiple-dose randomized clinical trial was conducted from August 11, 2021, to September 12, 2022, at 47 centers in the US and 8 in Canada. The study included a 12-week treatment period and a 4-week follow-up period. Key eligibility criteria for participants included age 18 to 70 years; a Psoriasis Area and Severity Index (PASI) score of 12 or greater; a Physician's Global Assessment score of 3 or greater; and a body surface area covered by plaque psoriasis of 10% or greater. Of 287 patients randomized, 259 (90.2%) received at least 1 dose of study treatment.
Intervention: Patients were randomly assigned (1:1:1:1:1) to receive zasocitinib at 2, 5, 15, or 30 mg or placebo orally, once daily, for 12 weeks.
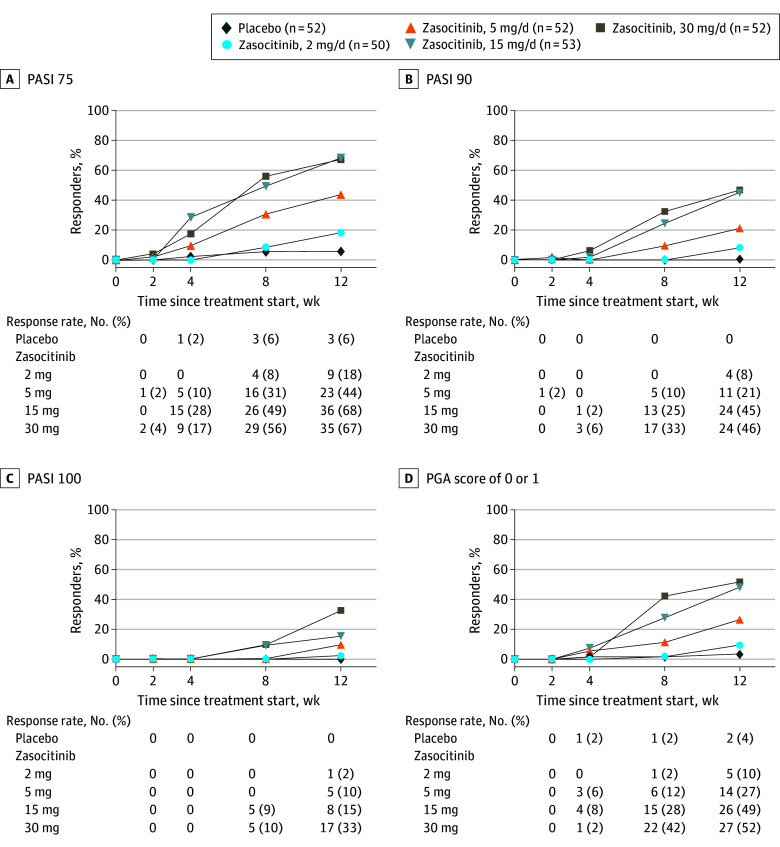
Main outcomes and measures: The primary efficacy end point was the proportion of patients achieving 75% or greater improvement in PASI score (PASI 75) at week 12. Secondary efficacy end points included PASI 90 and 100 responses. Safety was also assessed.
Results: In total, 259 patients were randomized and received treatment (mean [SD] age, 47 [13] years; 82 women [32%]). At week 12, PASI 75 was achieved for 9 (18%), 23 (44%), 36 (68%), and 35 (67%) patients receiving zasocitinib at 2, 5, 15, and 30 mg, respectively, and 3 patients (6%) receiving placebo. PASI 90 responses were consistent with PASI 75. PASI 100 demonstrated a dose response at all doses, with 17 patients (33%) achieving PASI 100 with zasocitinib, 30 mg. Treatment-emergent adverse events occurred for 23 patients (44%) receiving placebo and 28 (53%) to 31 (62%) patients receiving the 4 different doses of zasocitinib, with no dose dependency and no clinically meaningful longitudinal differences in laboratory parameters.
Conclusions and relevance: This randomized clinical trial found that potent and selective inhibition of TYK2 with zasocitinib at oral doses of 5 mg or more once daily resulted in greater skin clearance than placebo over 12 weeks.
Trial registration: ClinicalTrials.gov Identifier: NCT04999839.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
