

Decreasing chronic graft-versus-host disease rates in all populations
- PMID: 39167805
- PMCID: PMC11609357
- DOI: 10.1182/bloodadvances.2024012722
Decreasing chronic graft-versus-host disease rates in all populations
Abstract
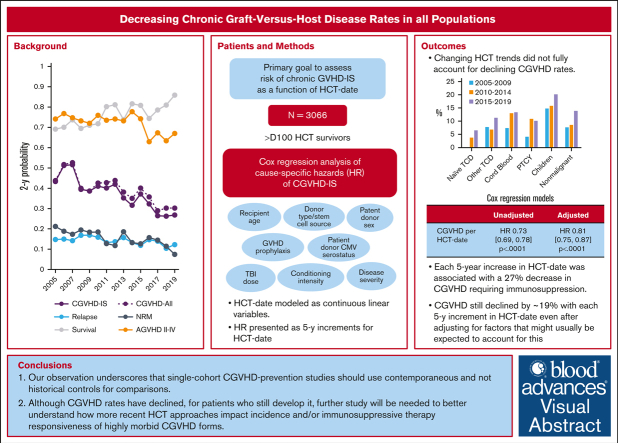
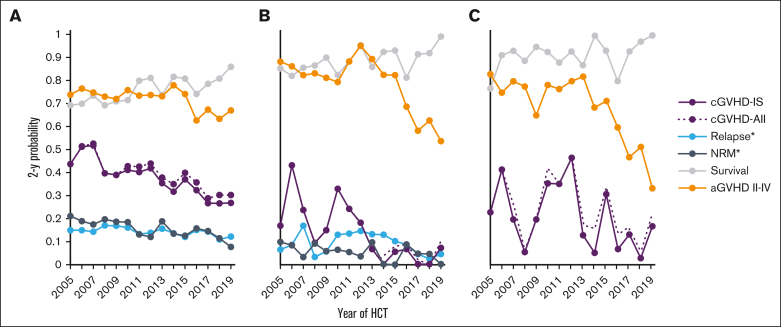
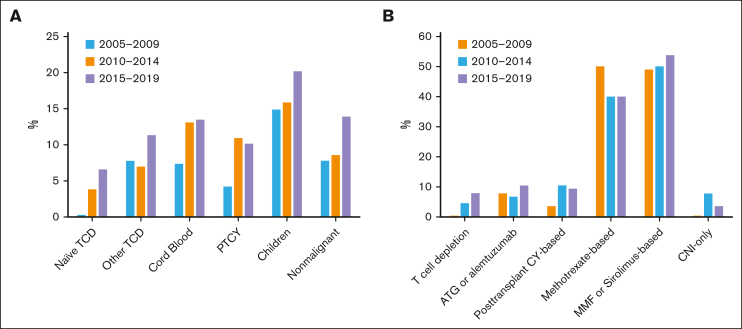
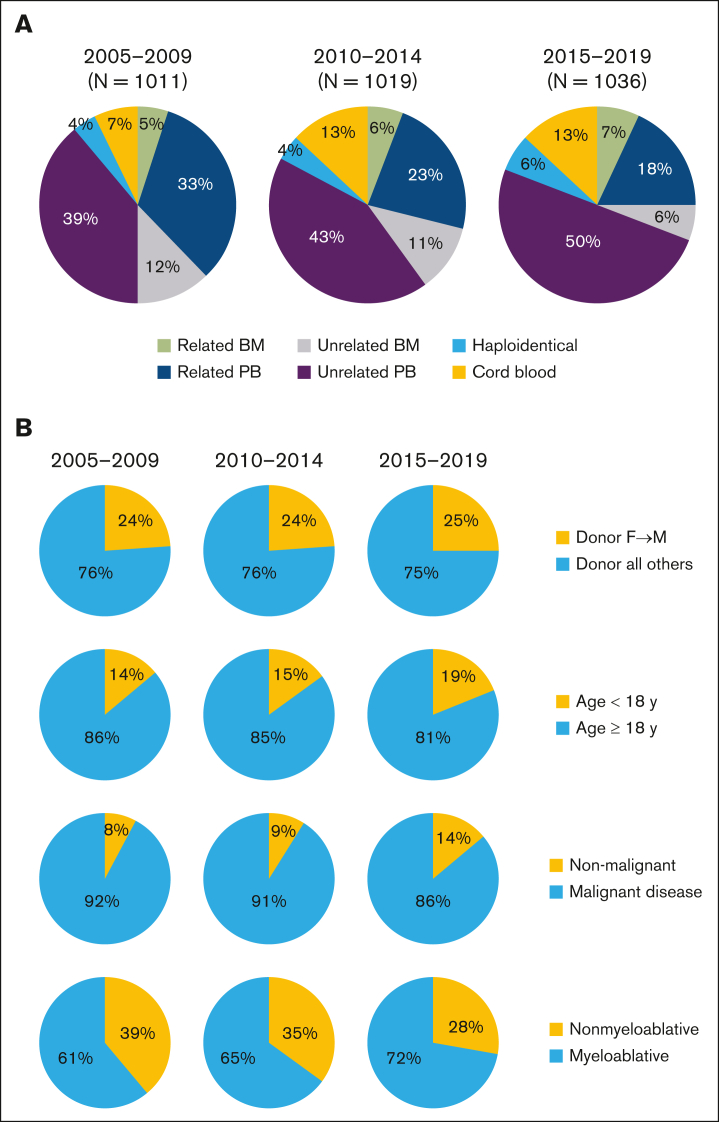
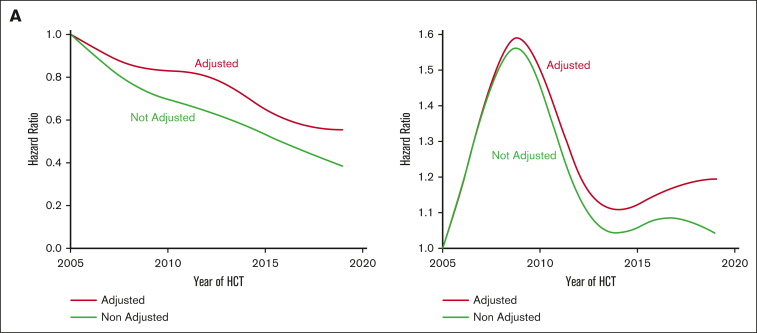
Since 2005, there has been a steady decline in chronic graft-versus-host disease (cGVHD) at the Fred Hutchinson Cancer Center. To better understand this phenomenon, we studied the risk of cGVHD requiring systemic immunosuppression (cGVHD-IS) as a function of hematopoietic cell transplantation (HCT) date in 3066 survivors from 2005 through 2019. Cox regression models were fit to assess associations of HCT date (as a continuous linear variable) with cause-specific hazards of cGVHD using unadjusted and adjusted models. Median follow-up for study subjects was 7.0 years (range, 1.0-17.2). Two-year probabilities of cGVHD-IS declined among all survivors from 45% to 52% (2005-2007) to ∼40% (2008-2012) and then further to ∼26% by 2017. A decline was also observed when the analysis was restricted to 502 pediatric survivors, with cGVHD-IS probabilities <10% since 2013. Among 305 adult and pediatric survivors who underwent transplantation for nonmalignant diseases, cGVHD rates showed greater fluctuation but remained <20% after 2016. Each 5-year increase in HCT date was associated with a 27% decrease in the cause-specific hazard of cGVHD (unadjusted hazard ratio [HR], 0.73; 95% confidence interval [CI], 0.68-0.78; P < .0001); the HR was 0.81 (95% CI, 0.75-0.87; P < .0001) even after adjusting for various factors (age, donor/stem-cell source, race, sex, conditioning intensity, GVHD prophylaxis, among others) that could lead to cGVHD reduction. The decline in cGVHD was not fully explained by demographic shifts and greater use of HCT approaches that are generally associated with lower cGVHD rates. This observation underscores that single-cohort cGVHD prevention studies should use contemporaneous and not historical controls for comparison.
© 2024 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
References
-
- Filipovich AH, Weisdorf D, Pavletic S, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant. 2005;11(12):945–956. - PubMed
-
- Gauthier J, Wu QV, Gooley TA. Cubic splines to model relationships between continuous variables and outcomes: a guide for clinicians [editorial] Bone Marrow Transplant. 2020;55(4):675–680. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
