

Incidence and risk factors for first and recurrent ICD shock therapy in patients with an implantable cardioverter defibrillator
- PMID: 39168942
- PMCID: PMC11832632
- DOI: 10.1007/s10840-024-01873-0
Incidence and risk factors for first and recurrent ICD shock therapy in patients with an implantable cardioverter defibrillator
Abstract
Background: Advances in medical treatment and outcomes in implantable cardioverter-defibrillator (ICD) recipients incentivize a need for improved candidate selection and identification of risk factors for ICD therapy. We examined contemporary rates of and risk factors for ICD therapy.
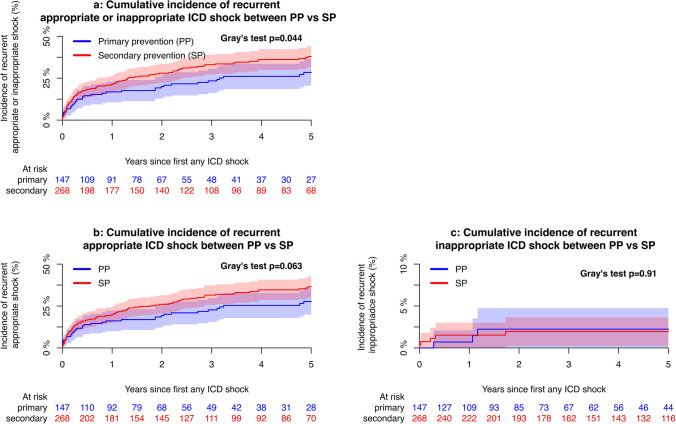
Methods: Patients with ICD for primary (PP) or secondary prevention (SP), implanted between January 2010 and December 2020, were followed for appropriate and inappropriate incident and recurrent shock.
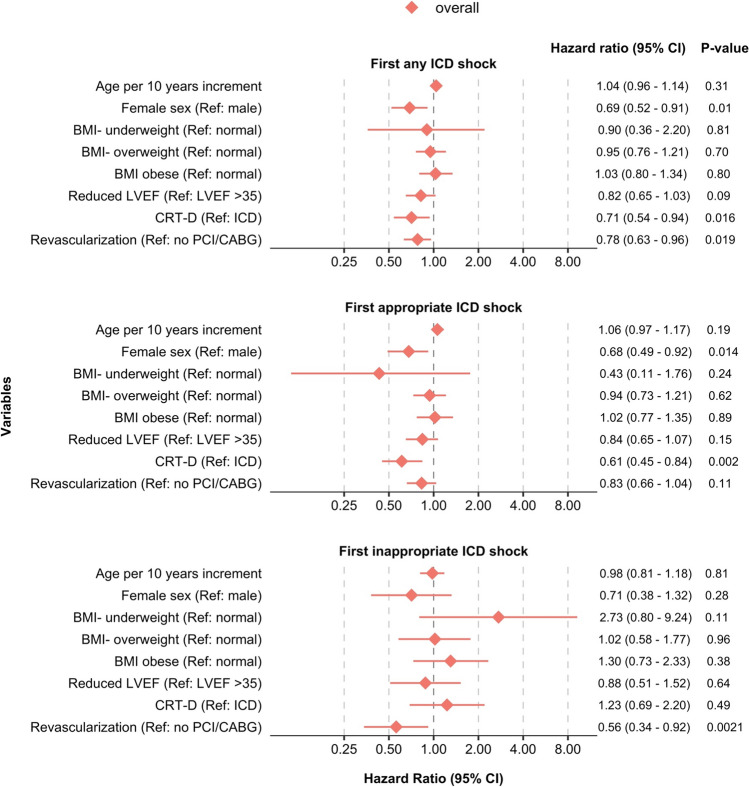
Results: Overall, 2998 patients (mean age 61.8 ± 12.7 years, 20% female, 73% ICD carriers, and 47.1% SP) were analyzed with a median follow-up of 4.3 (interquartile range (IQR) 2.1-7.4) years. A total of 426/2998 (14.2%) patients had shock; 364/2998 (12.1%) had appropriate and 82/2998 (2.7%) inappropriate shock, with annualized event rates of 2.34 (2.11-2.59) and 0.49 (0.39-0.61) per 100 person-years, respectively. Of those with shock, 133/364 (36.5%) experienced recurrent appropriate shock and 8/364 (2.2%) received recurrent inappropriate shock, with event rates of 10.57 (8.85-12.53) and 0.46 (0.20-0.92), respectively. In multivariable analyses, female sex was associated with a reduced risk of incident appropriate shock (hazard ratio 0.69 [95% confidence interval 0.52; 0.91]). Of other variables, only revascularization status was associated with recurrent appropriate shock in PP, and CRT-D with recurrent appropriate shock in the overall cohort.
Conclusion: One in eight ICD recipients received appropriate shock 2-7 years after guideline-directed implantation. More than one-third of patients with a first shock experienced recurrent shock. Few clinical variables showed potential in predicting shocks, illustrating a need for more advanced tools to select candidates for implantation.
Keywords: ICD-therapy; Implantable cardioverter defibrillator; Recurrent shock; Risk factors; Ventricular arrhythmia.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: Frodi, Xing, Spona, and Risum declare no conflicting interests. Jacobsen has given lectures for Medtronic. Diederichsen is a consultant for Bristol Myers Squibb / Pfizer, Acesion Pharma, Vital Beats and Cortrium. He has received speaker fees from Bristol Myers Squibb / Pfizer and Bayer. Svendsen is a member of an advisory board of Vital Beats and Medtronic and has received speaker’s fee and an unrestricted research grant from Medtronic, independently to this study.
Figures


References
-
- Zeppenfeld K, Tfelt-Hansen J, de Riva M, Winkel BG, Behr ER, Blom NA, ESC Scientific Document Group. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. 2022;43(40):3997–4126. 10.1093/eurheartj/ehac262. - PubMed
-
- Gómez-Mesa JE, Márquez-Murillo M, Figueiredo M, Berni A, Jerez AM, Núñez-Ayala E, Romero A. Inter-American Society of Cardiology (CIFACAH-ELECTROSIAC) and Latin-American Heart Rhythm Society (LAHRS): multidisciplinary review on the appropriate use of implantable cardiodefibrillator in heart failure with reduced ejection fraction. J Interv Cardiac Electrophysiol: An Int J Arrhythmias Pacing. 2023;66(5):1211–29. 10.1007/s10840-022-01425-4. - PMC - PubMed
-
- Shen L, Jhund PS, Petrie MC, Claggett BL, Barlera S, Cleland JGF, McMurray JJV. Declining risk of sudden death in heart failure. New England J Med. 2017;377(1):41–51. 10.1056/NEJMoa1609758. - PubMed
-
- Gierula J, Paton MF, Witte KK. Advances in cardiac resynchronization and implantable cardioverter/defibrillator therapy: Medtronic Cobalt and Crome. Future Cardiol. 2021;17(4):609–18. 10.2217/fca-2020-0117. - PubMed
-
- Ågesen FN, Lynge TH, Blanche P, Banner J, Prescott E, Jabbari R, Tfelt-Hansen J. Temporal trends and sex differences in sudden cardiac death in the Copenhagen City Heart Study. Heart (British Cardiac Society). 2021;107(16):1303–9. 10.1136/heartjnl-2020-318881. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
