

A gut microbiota rheostat forecasts responsiveness to PD-L1 and VEGF blockade in mesothelioma
- PMID: 39168966
- PMCID: PMC11339264
- DOI: 10.1038/s41467-024-49842-5
A gut microbiota rheostat forecasts responsiveness to PD-L1 and VEGF blockade in mesothelioma
Abstract
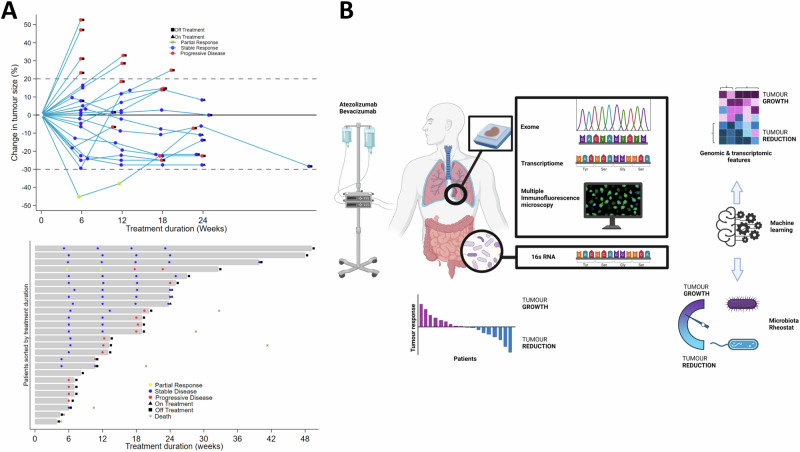
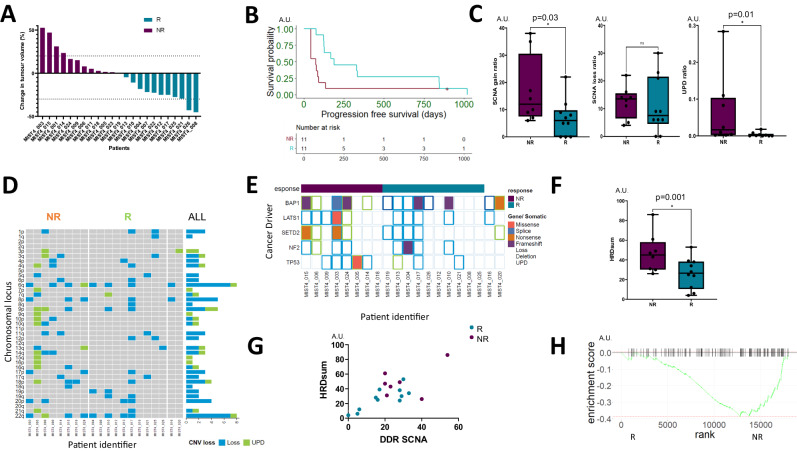
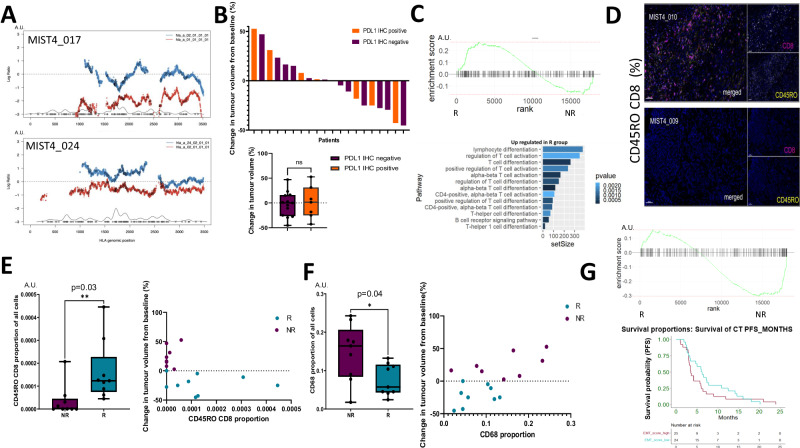
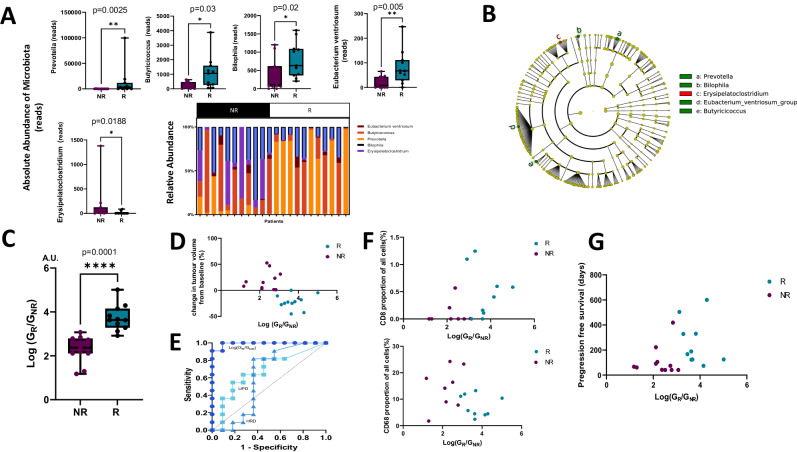
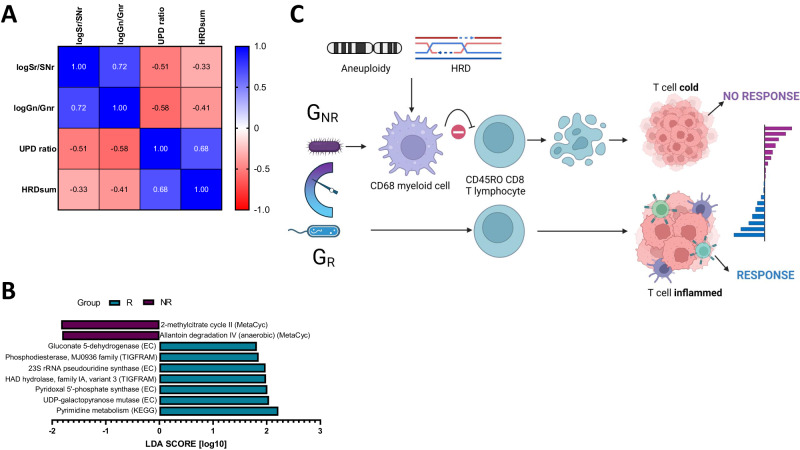
Malignant mesothelioma is a rare tumour caused by asbestos exposure that originates mainly from the pleural lining or the peritoneum. Treatment options are limited, and the prognosis is dismal. Although immune checkpoint blockade (ICB) can improve survival outcomes, the determinants of responsiveness remain elusive. Here, we report the outcomes of a multi-centre phase II clinical trial (MiST4, NCT03654833) evaluating atezolizumab and bevacizumab (AtzBev) in patients with relapsed mesothelioma. We also use tumour tissue and gut microbiome sequencing, as well as tumour spatial immunophenotyping to identify factors associated with treatment response. MIST4 met its primary endpoint with 50% 12-week disease control, and the treatment was tolerable. Aneuploidy, notably uniparental disomy (UPD), homologous recombination deficiency (HRD), epithelial-mesenchymal transition and inflammation with CD68+ monocytes were identified as tumour-intrinsic resistance factors. The log-ratio of gut-resident microbial genera positively correlated with radiological response to AtzBev and CD8+ T cell infiltration, but was inversely correlated with UPD, HRD and tumour infiltration by CD68+ monocytes. In summary, a model is proposed in which both intrinsic and extrinsic determinants in mesothelioma cooperate to modify the tumour microenvironment and confer clinical sensitivity to AtzBev. Gut microbiota represent a potentially modifiable factor with potential to improve immunotherapy outcomes for individuals with this cancer of unmet need.
© 2024. The Author(s).
Conflict of interest statement
D.A.F. reports grants from Aldeyra, Astex Therapeutics, Bayer, BMS and Boehringer Ingelheim, Owkin; non-financial support from BerGenBio, Clovis, Eli Lilly, MSD, Roche, and Tesaro GSK; personal fees from Aldeyra, Cambridge Clinical Laboratories, Ikena, Opna Bio, Owkin, RS Oncology, Roche, MSD, during the conduct of the study. All other authors declare no competing interests.
Figures
References
-
- Baas, P. et al. First-line nivolumab plus ipilimumab in unresectable malignant pleural mesothelioma (CheckMate 743): a multicentre, randomised, open-label, phase 3 trial. Lancet397, 375–386 (2021). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
