

Different diabetogenic effect of statins according to intensity and dose in patients with acute myocardial infarction: a nationwide cohort study
- PMID: 39169014
- PMCID: PMC11339444
- DOI: 10.1038/s41598-024-67585-7
Different diabetogenic effect of statins according to intensity and dose in patients with acute myocardial infarction: a nationwide cohort study
Abstract
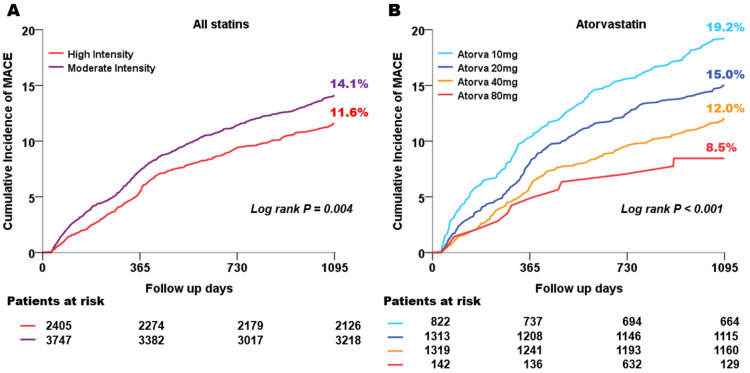
Statin is crucial for acute myocardial infarction (AMI) patients. However, the risk of new-onset diabetes mellitus (NODM) associated with statin is a concern. This study aimed to determine the incremental diabetogenic effects of statins according to their intensity and dose in AMI patients undergoing percutaneous coronary intervention (PCI). Among 13,104 patients enrolled in the Korea AMI Registry between 2011 and 2015, 6152 patients without diabetes mellitus (DM) who underwent PCI and received moderate-to-high-intensity atorvastatin and rosuvastatin were selected for the study. The endpoints were NODM and major adverse cardiovascular events (MACE), composite of all-cause mortality, recurrent MI, and revascularization up to 3 years. Among the participants, 3747 and 2405 received moderate- and high-intensity statins, respectively. The Kaplan-Meier curves demonstrated a higher incidence of NODM in patients with high-intensity statins than those with moderate-intensity. High-intensity statin was a significant predictor of NODM after adjusting for other co-variables (HR = 1.316, 95% CI 1.024-1.692; P < 0.032). Higher dose of rosuvastatin was associated with a higher cumulative incidence of NODM, but this dose-dependency was not apparent with atorvastatin. Cumulative incidence of MACE decreased dose-dependently only with atorvastatin. High-intensity statin was associated with a higher cumulative incidence of NODM in AMI patients, and this association was more evident in rosuvastatin. The different diabetogenic effects of the two statins provide supporting evidence for understanding the nuanced nature of statin treatment in relation to NODM.
Keywords: Acute myocardial infarction; New-onset diabetes mellitus; Statin intensity.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Ridker, P. M. et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N. Engl. J. Med.359, 2195–2207. 10.1056/NEJMoa0807646 (2008). - PubMed
-
- Sacks, F. M. et al. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events Trial investigators. New Engl. J. Med.335, 1001–1009. 10.1056/nejm199610033351401 (1996). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
