

Molecular classification to refine surgical and radiotherapeutic decision-making in meningioma
- PMID: 39169220
- PMCID: PMC11564112
- DOI: 10.1038/s41591-024-03167-4
Molecular classification to refine surgical and radiotherapeutic decision-making in meningioma
Abstract
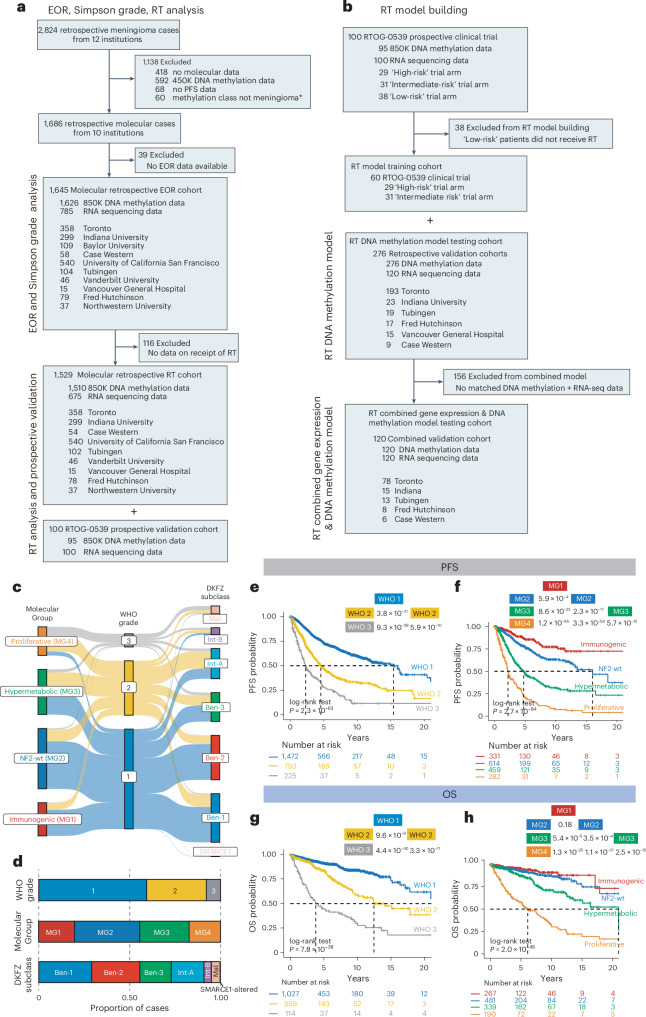
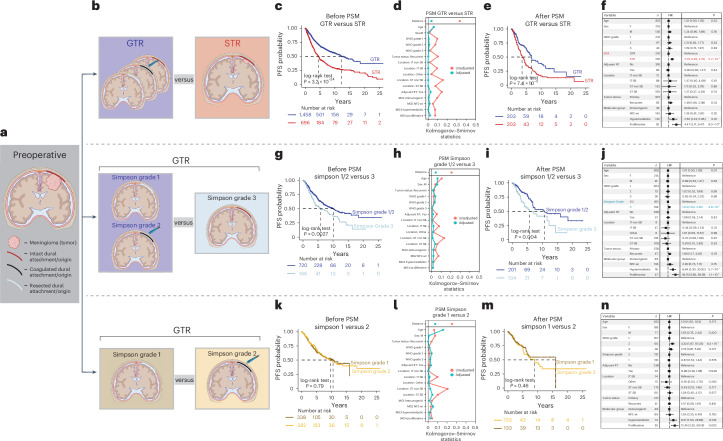
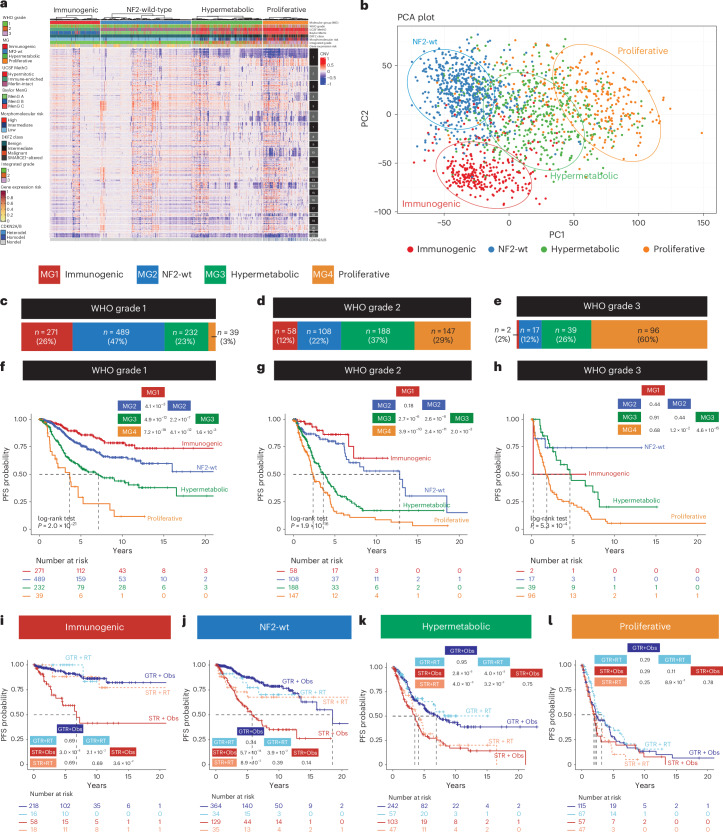
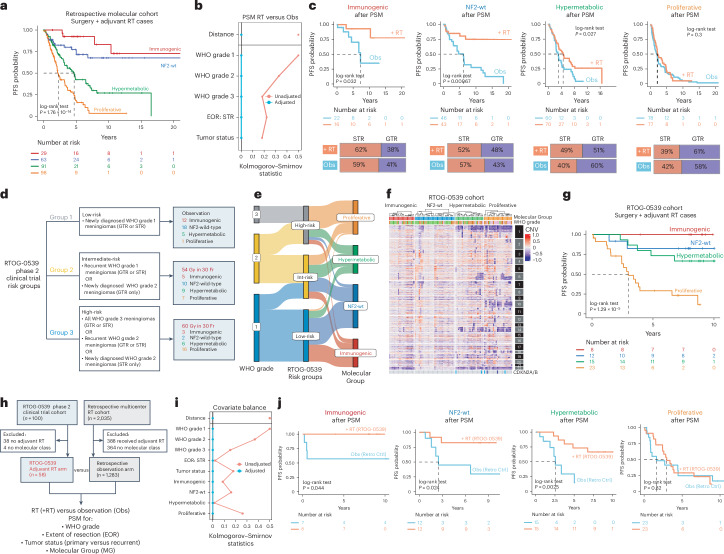
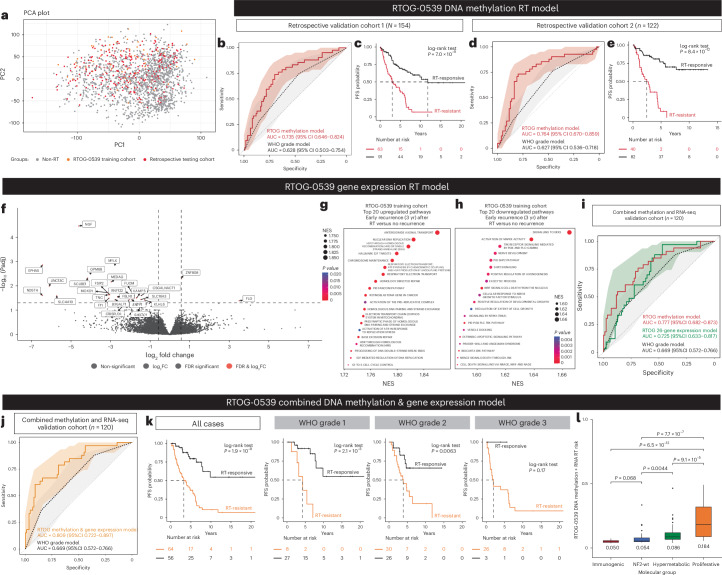
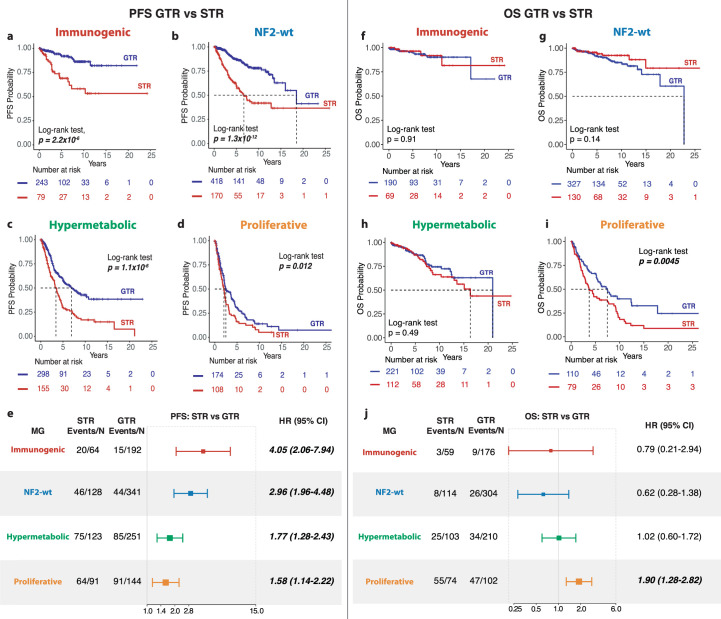
Treatment of the tumor and dural margin with surgery and sometimes radiation are cornerstones of therapy for meningioma. Molecular classifications have provided insights into the biology of disease; however, response to treatment remains heterogeneous. In this study, we used retrospective data on 2,824 meningiomas, including molecular data on 1,686 tumors and 100 prospective meningiomas, from the RTOG-0539 phase 2 trial to define molecular biomarkers of treatment response. Using propensity score matching, we found that gross tumor resection was associated with longer progression-free survival (PFS) across all molecular groups and longer overall survival in proliferative meningiomas. Dural margin treatment (Simpson grade 1/2) prolonged PFS compared to no treatment (Simpson grade 3). Molecular group classification predicted response to radiotherapy, including in the RTOG-0539 cohort. We subsequently developed a molecular model to predict response to radiotherapy that discriminates outcome better than standard-of-care classification. This study highlights the potential for molecular profiling to refine surgical and radiotherapy decision-making.
© 2024. The Author(s).
Conflict of interest statement
Figures






References
-
- Vernooij, M. W. et al. Incidental findings on brain MRI in the general population. N. Engl. J. Med.357, 1821–1828 (2007). - PubMed
-
- Gallagher, M. J., Jenkinson, M. D., Brodbelt, A. R., Mills, S. J. & Chavredakis, E. WHO grade 1 meningioma recurrence: are location and Simpson grade still relevant? Clin. Neurol. Neurosurg.141, 117–121 (2016). - PubMed
-
- Gousias, K., Schramm, J. & Simon, M. The Simpson grading revisited: aggressive surgery and its place in modern meningioma management. J. Neurosurg.125, 551–560 (2016). - PubMed
