

Performance status improvement and advances in systemic treatment after brain metastases resection: a retrospective single-center cohort study of non-small cell lung cancer patients
- PMID: 39169327
- PMCID: PMC11337764
- DOI: 10.1186/s12885-024-12798-2
Performance status improvement and advances in systemic treatment after brain metastases resection: a retrospective single-center cohort study of non-small cell lung cancer patients
Abstract
Background: Brain metastasis (BrM) is prevalent among patients with NSCLC, and surgical resection of BrM constitutes a promising treatment strategy for local management and histopathological diagnosis, although it is offered for a select group of patients. Limited information exists concerning the improvement in performance status (PS) following BrM resection or the outcomes stratified by subsequent systemic therapy.
Methods: We conducted a retrospective single-center cohort study including NSCLC patients with surgically resected BrM and focused on the improvement in PS and subsequent therapy after BrM resection.
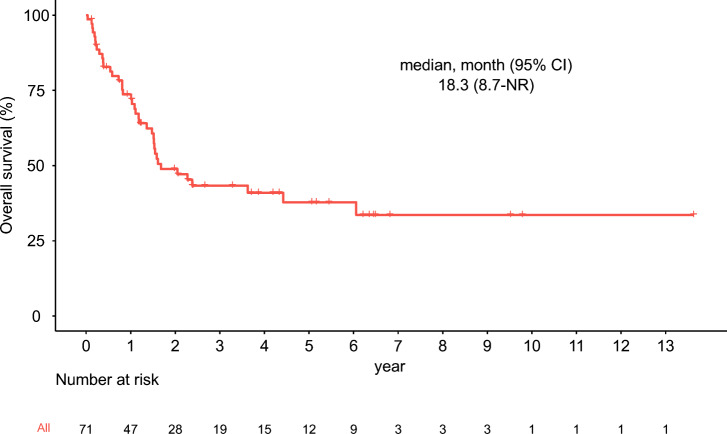
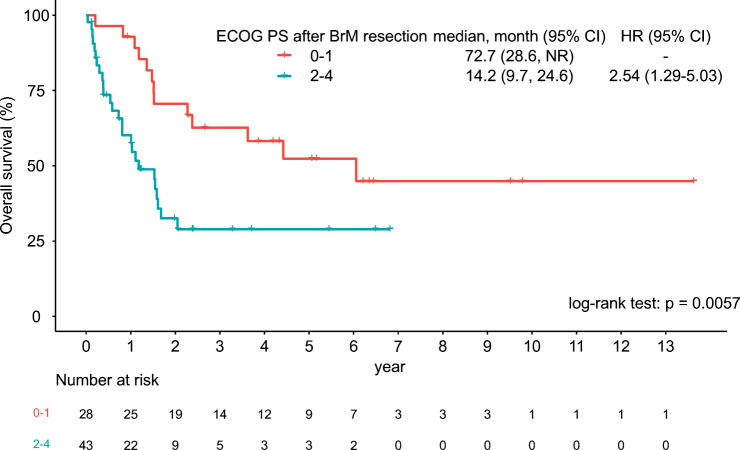
Results: 71 patients were included, and the median overall survival was 18.3 months (95% confidence interval [95% CI]: 8.7, not reached). Patients with NSCLC who underwent surgical resection of BrM showed significant improvement in PS (18% and 39% showed ECOG PS of 0-1, before and after BrM resection, respectively [p = 0.006]), and patients with PS improvement were younger than those with PS unimprovement (median, 62 years versus 66 years; p = 0.041). Regarding subsequent systemic therapy after BrM resection, 21 patients (30%) received cytotoxic chemotherapy, 14 patients (20%) received tyrosine kinase inhibitors (TKIs), 3 patients (4%) received immune checkpoint inhibitors (ICIs), and 21 patients (30%) received no subsequent therapy. The survival outcomes of patients stratified by subsequent systemic treatments suggested the tendency that those who received TKI or ICI showed better survival outcomes, although a small number of patients hindered statistical comparisons.
Conclusions: We describe the outcomes of patients with NSCLC who underwent surgical resection of BrM, revealing that younger patients were more likely to anticipate improvement in PS, and patients who received TKI or ICI after BrM resection tended to exhibit a more preferable prognosis.
Keywords: Brain metastasis; Immune-checkpoint inhibitor; Non-small cell lung cancer; Performance status; Surgical resection.
© 2024. The Author(s).
Conflict of interest statement
YA reports grants from Philips, Otsuka, Chugai, Nihon Medi-Physics, Daiichi Sankyo, Stryker, Eisai, Japan Blood Products Organization, Ono Pharmaceutical, Taiho Pharma, Sumitomo Dainippon Pharma, Astellas Pharma, Incyte Biosciences, and Servier and personal fees from Nippon Kayaku, Novocure, UCB Japan, Ono Pharmaceutical, Brainlab, Merck, Chugai, Eisai, Daiichi Sankyo, Carl Zeiss, and Nihon Medi-Physics. The other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7–33. 10.3322/caac.21708. - PubMed
-
- Barnholtz-Sloan JS, Sloan AE, Davis FG, Vigneau FD, Lai P, Sawaya RE. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J Clin Oncol off J Am Soc Clin Oncol. 2004;22(14):2865–72. 10.1200/JCO.2004.12.149. - PubMed
-
- Nayak L, Lee EQ, Wen PY. Epidemiology of brain metastases. Curr Oncol Rep. 2012;14(1):48–54. 10.1007/s11912-011-0203-y. - PubMed
-
- Kim M, Suh CH, Lee SM, et al. Development of Brain metastases in patients with Non-small Cell Lung Cancer and No Brain metastases at initial staging evaluation: cumulative incidence and risk factor analysis. AJR Am J Roentgenol. 2021;217(5):1184–93. 10.2214/AJR.21.25787. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
