

A Novel and Effective Surgical Technique for Reconstruction of Extensor Mechanism with Iliotibial Band Tendon Graft After Patellectomy for Primary Patella Tumor
- PMID: 39170664
- PMCID: PMC11333392
- DOI: 10.1007/s43465-024-01190-8
A Novel and Effective Surgical Technique for Reconstruction of Extensor Mechanism with Iliotibial Band Tendon Graft After Patellectomy for Primary Patella Tumor
Abstract
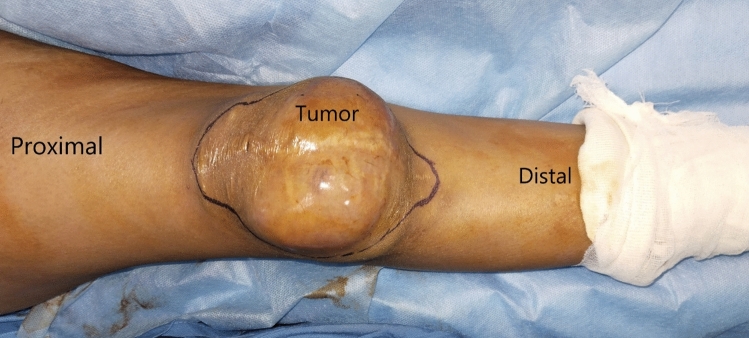
Background: Amongst primary patella tumor Campanacci grade 3 tumor of Giant cell tumor of bone (GCTB) and malignant tumors requires patellectomy. We had a patient with huge recurrent GCTB of patella with involvement of skin. We reconstructed extensor mechanism of Knee with long iliotibial band (ITB) tendon graft.
Material and methods: After patellectomy, we harvested long ITB graft (length 22 cm; width proximally 6 cm, distally 1.5 cm) through patellectomy wound and small "L" shaped incision proximally. We passed ITB graft from patella tendon and quadriceps tendon in figure of 8 manner and sutured it back to itself and host tendon with fiber Wire and closed both the wounds primarily. We started ROM and quadriceps strengthening in graded manner. We measured functional outcome with Musculoskeletal Tumour Society (MSTS) scoring system.
Results: There were no post-operative complications. At 10 weeks follow up, patient had no extension lag and knee ROM was 90°. At final follow up of 7 months patient regained pre-operative functional status without knee instability. Her MSTS score was 30 and she was disease free.
Conclusion: Reconstruction of extensor mechanism of knee with ITB graft doesn't have donor site morbidity and gives excellent function with graded physiotherapy protocol.
Keywords: Extensor defect; Giant cell tumor of Patella; Iliotibial band graft; Knee extensor mechanism reconstruction; Tumor of patella.
© Indian Orthopaedics Association 2024. Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Conflict of interest statement
Conflict of interestThe authors have no relevant financial or non-financial interests to disclose.
Figures






References
LinkOut - more resources
Full Text Sources