

Endoscopic Versus Surgical Treatment for Ampullary Lesions: A Systematic Review With Meta-Analysis
- PMID: 39170988
- PMCID: PMC11337076
- DOI: 10.7759/cureus.65076
Endoscopic Versus Surgical Treatment for Ampullary Lesions: A Systematic Review With Meta-Analysis
Abstract
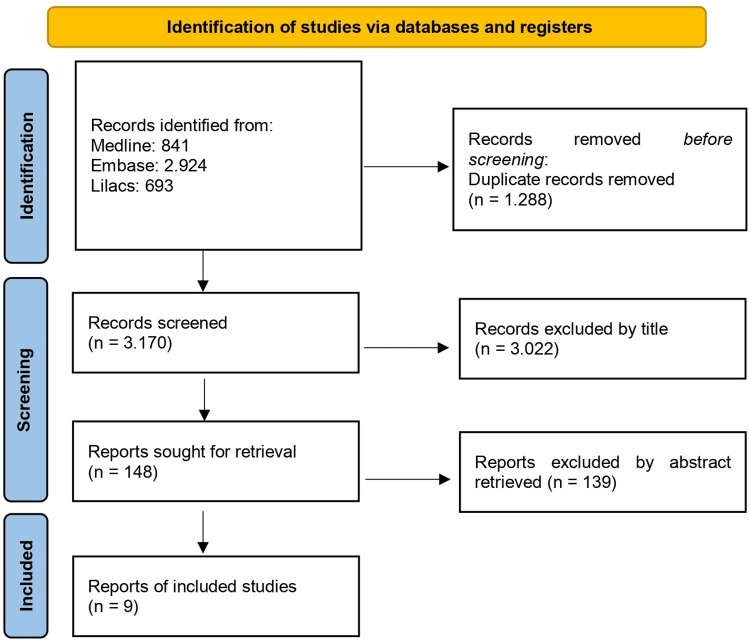
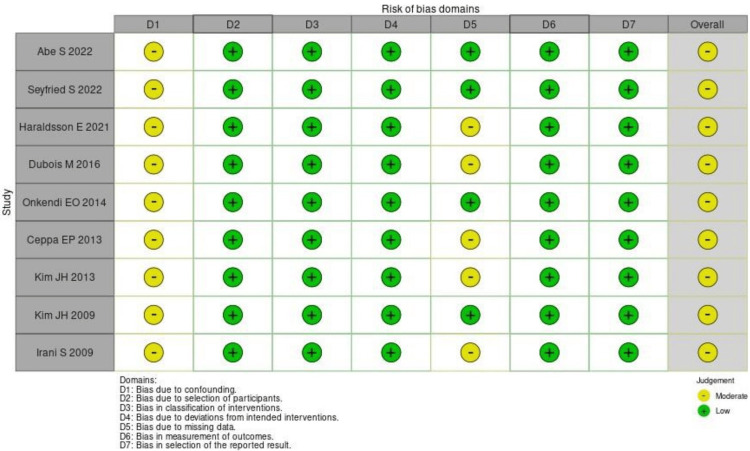
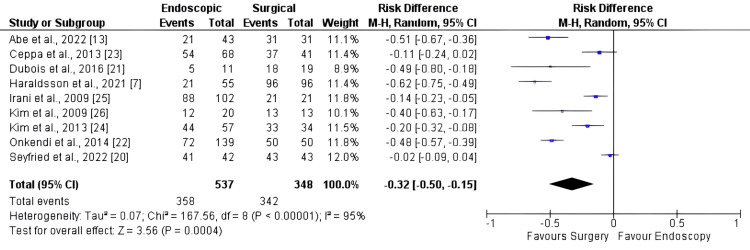
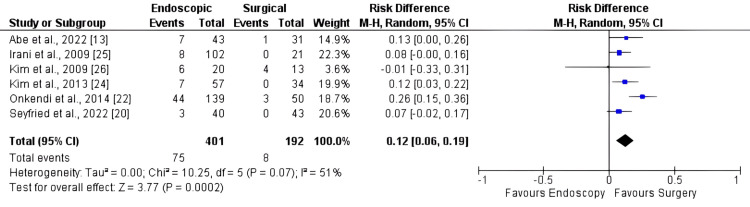
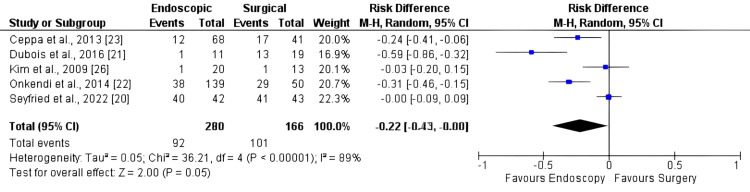
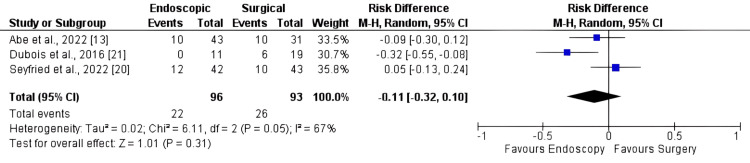
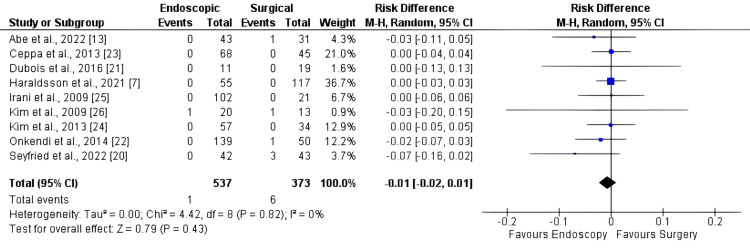
Ampullary lesions (ALs) can be treated through either an endoscopic approach (EA) or a surgical approach (SA). However, it is important to note that EAs carry a significant risk of incomplete resection, while opting for surgical interventions can result in substantial morbidity. We performed a systematic review and meta-analysis for R0 resection, recurrence, adverse events in general, major adverse events, mortality, and length of hospital stay between SAs and EAs. Electronic databases were searched from inception to 2023. We identified nine independent studies. The risk difference was -0.32 (95% CI: -0.50, -0.15; p <0.001) for R0, 0.12 (95% CI: 0.06, 0.19; p < 0.001) for recurrence, -0.22 (95% CI: -0.43, 0.00; p 0.05) for overall adverse events, -0.11 (95% CI: -0.32, 0.10; p = 0.31) for major complications, -0.01 (95% CI: -0.02, 0.01; p = 0.43) for mortality, and -14.69 (95% CI: -19.91, -9.47; p < 0.001) for length of hospital stay. As expected, our data suggest a higher complete resection rate and lower recurrence from surgical interventions, but this is associated with an elevated risk of adverse events and a longer hospital stay.
Keywords: ampulla of vater; ampullary adenoma; duodenal neoplasms; endoscopy; pancreaticoduodenectomy; surgery.
Copyright © 2024, Baroni et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
-
- Endoscopic management of ampullary tumors: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Vanbiervliet G, Strijker M, Arvanitakis M, et al. Endoscopy. 2021;53:429–448. - PubMed
-
- Endoscopic resection of benign tumors of the duodenal papilla without and with intraductal growth. Bohnacker S, Seitz U, Nguyen D, et al. Gastrointest Endosc. 2005;62:551–560. - PubMed
-
- Endoscopic ampullectomy: a technical review. Espinel J, Pinedo E, Ojeda V, Guerra Del Río M. Rev Esp Enferm Dig. 2016;108:271–278. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous