

Cardiocerebral Infarction Presenting in a Neurosurgical Emergency: A Case Report and Literature Review
- PMID: 39171037
- PMCID: PMC11338544
- DOI: 10.7759/cureus.65124
Cardiocerebral Infarction Presenting in a Neurosurgical Emergency: A Case Report and Literature Review
Abstract
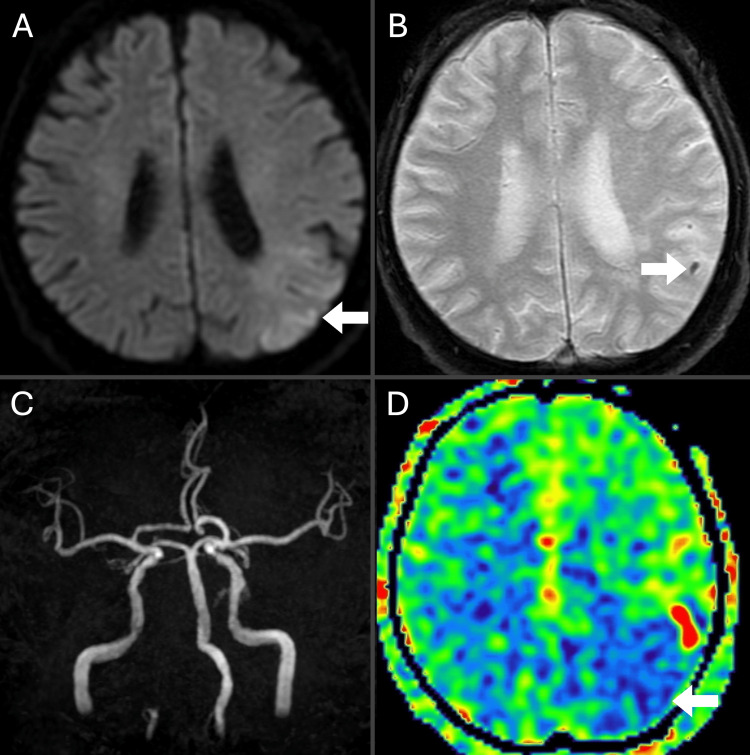
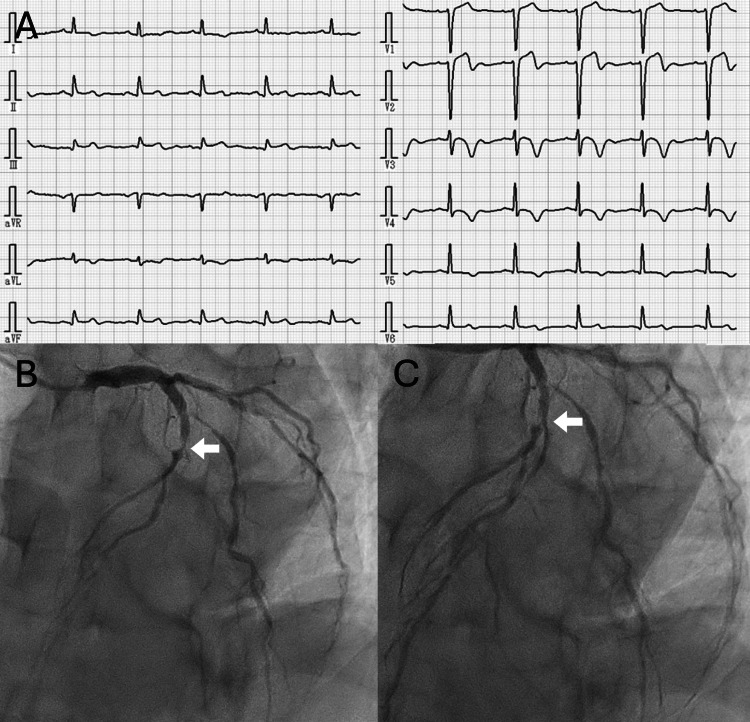
Cardiocerebral infarction (CCI), the simultaneous occurrence of acute ischemic stroke and acute myocardial infarction (AMI), is a rare but critical condition. However, the optimal treatment strategy, particularly regarding the use of tissue plasminogen activator (t-PA), remains unclear. This case report describes a patient with CCI diagnosed during a neurosurgical emergency. A 67-year-old man with a history of hypertension presented with sudden right hemiparesis and sensory aphasia 30 minutes prior to hospital arrival. Diffusion-weighted magnetic resonance imaging revealed acute cerebral infarction in the left middle cerebral artery territory but without large-vessel occlusion. Routine electrocardiography (ECG) showed ST-T elevation in leads V1, V2, II, III, and aVF (augmented vector foot). Subsequent blood tests confirmed positive troponin T and elevated creatine kinase levels. Despite the absence of reported AMI symptoms, the patient received a diagnosis of CCI. Due to the uncertain time of AMI onset and to expedite transfer to the percutaneous coronary intervention (PCI) unit, t-PA administration was withheld. Upon transfer, dual antiplatelet therapy with aspirin (200 mg) and clopidogrel (300 mg) was initiated. Emergency coronary angioplasty successfully treated a 99% stenosis of the left anterior descending artery (#7). The patient's post-procedure course was uneventful. After 18 days, he was transferred to a rehabilitation hospital with a modified Rankin Scale score of 3. This case highlights the importance of routine 12-lead ECG in neurosurgical emergencies, regardless of presenting symptoms like chest pain. While guidelines support the use of t-PA in CCI, its administration requires careful consideration due to specific risks, including cardiac rupture and limitations on antithrombotic therapy within the first 24 hours.
Keywords: 12-lead ecg; acute ischemic stroke; acute myocardial infarction; cardiocerebral infarction; t-pa; thrombolysis.
Copyright © 2024, Kume et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Concomitant acute right ventricular infarction and ischemic cerebrovascular stroke; possible explanations. Omar HR, Fathy A, Rashad R, Helal E. https://pubmed.ncbi.nlm.nih.gov/20977759/ Int Arch Med. 2010;3:25. - PMC - PubMed
-
- Trends in the incidence of the free wall cardiac rupture in acute myocardial infarction. Observational study: experience of a single center. Sobkowicz B, Lenartowska L, Nowak M, et al. https://pubmed.ncbi.nlm.nih.gov/16358958/ Rocz Akad Med Bialymst. 2005;50:161–165. - PubMed
-
- Myocardial infarction following intravenous thrombolysis for acute ischemic stroke: case report and literature review. Mannino M, Asciutto S, Terruso V, Gammino M, Cellura MG, Monaco S. J Stroke Cerebrovasc Dis. 2017;26:0–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous