

Community-level bystander treatment and outcomes for witnessed out-of-hospital cardiac arrest in the state of Connecticut
- PMID: 39171330
- PMCID: PMC11338120
- DOI: 10.1016/j.resplu.2024.100727
Community-level bystander treatment and outcomes for witnessed out-of-hospital cardiac arrest in the state of Connecticut
Abstract
Background: Prior reports have demonstrated underutilization of bystander cardiopulmonary resuscitation (CPR) and automated external defibrillator (AED) use in patients with witnessed out-of-hospital cardiac arrest (OHCA) in Connecticut. This study aimed to identify community-level risk factors that contribute to low rates of bystander intervention to improve statewide OHCA outcomes.
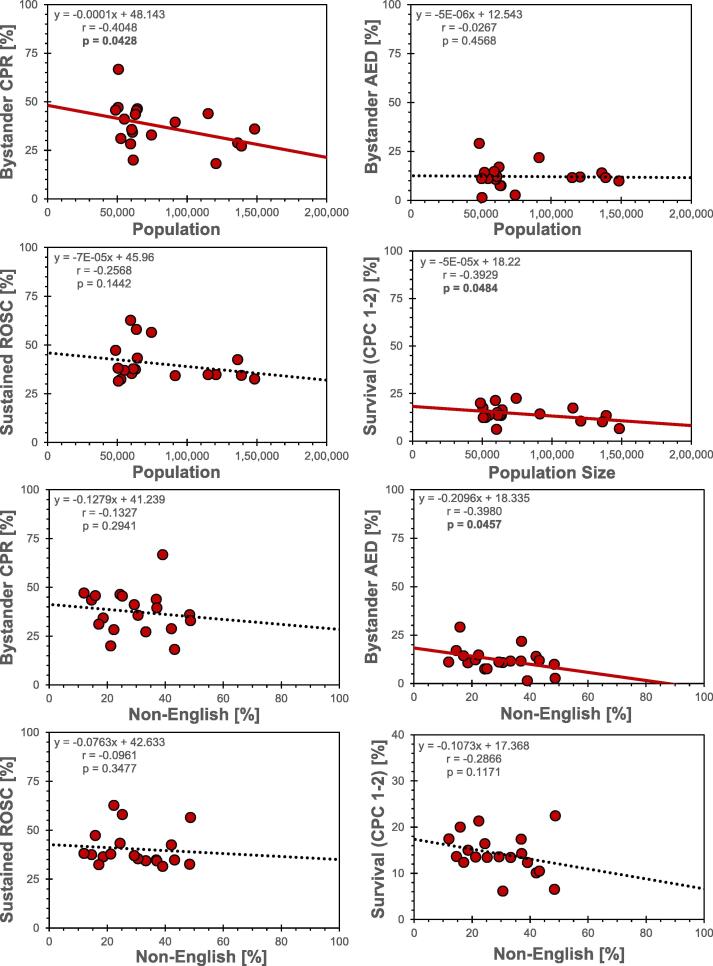
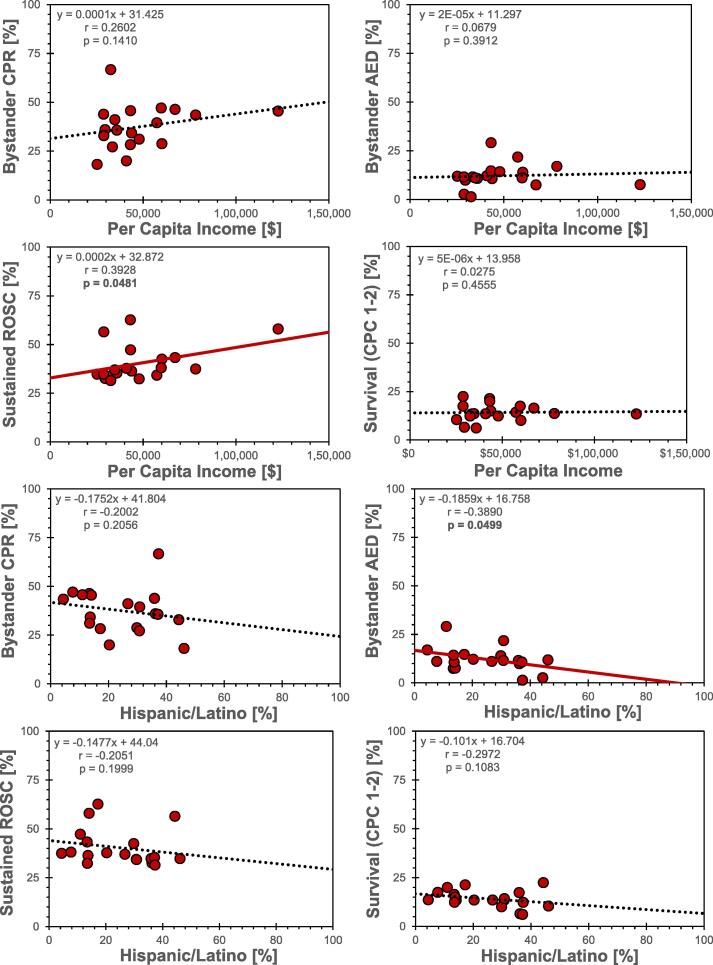
Methods: We analyzed 2,789 adult patients with witnessed, non-traumatic OHCA submitted to the Connecticut Cardiac Arrest Registry to Enhance Survival (CARES) between 2013-2022. Patients were grouped by zip code, and associated municipal characteristics were acquired from 2022 United States Census Bureau data. Use of bystander CPR, attempted bystander AED defibrillation, and patient survival with favorable neurological function were determined for 19 of the 20 most populous cities and towns. Pearson correlation tests and linear regression were used to determine associations between OHCA treatment and outcomes with population size, racial/ethnic demographics, language use, income, and educational level.
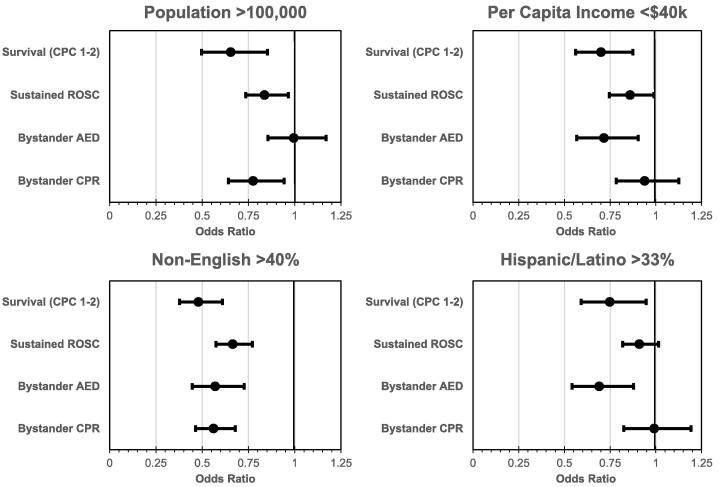
Results: Bystander CPR was lower in municipalities with population size > 100,000 and in communities where > 40% of residents are non-English-speaking. AED use was also lower in these municipalities, as well as those with per capita incomes < $40,000 or > 1/3 Hispanic residents. Communities with populations > 100,000, > 40% non-English-speaking, per capita income < $40,000, and > 1/3 Hispanic residents were all associated with lower survival rates.
Conclusions: OHCA pre-hospital treatment and outcomes vary significantly by municipality in Connecticut. Community outcomes might be improved by specifically targeting urban population centers and Hispanic communities with culturally sensitive, low, or no-cost CPR and AED educational programs, using instructional languages other than English.
Keywords: Bystander intervention; Cardiopulmonary resuscitation; Community health; Health disparities; Out-of-hospital cardiac arrest; Social determinants of health.
© 2024 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Racial and ethnic disparities in the treatment and outcomes for witnessed out-of-hospital cardiac arrest in Connecticut.Resuscitation. 2023 Jul;188:109850. doi: 10.1016/j.resuscitation.2023.109850. Epub 2023 May 23. Resuscitation. 2023. PMID: 37230326
-
Out-of-hospital cardiac arrest surveillance --- Cardiac Arrest Registry to Enhance Survival (CARES), United States, October 1, 2005--December 31, 2010.MMWR Surveill Summ. 2011 Jul 29;60(8):1-19. MMWR Surveill Summ. 2011. PMID: 21796098
-
Community Variations in Out-of-Hospital Cardiac Arrest Care and Outcomes in Texas.Prehosp Emerg Care. 2022 Mar-Apr;26(2):204-211. doi: 10.1080/10903127.2021.1907007. Epub 2021 Apr 13. Prehosp Emerg Care. 2022. PMID: 33779479
-
CPR and AEDs save lives: insuring CPR--AED education and CPR--AED access in schools.Curr Opin Pediatr. 2020 Oct;32(5):641-645. doi: 10.1097/MOP.0000000000000941. Curr Opin Pediatr. 2020. PMID: 32833798 Review.
-
Impact of community-based interventions on out-of-hospital cardiac arrest outcomes: a systematic review and meta-analysis.Sci Rep. 2023 Jun 23;13(1):10231. doi: 10.1038/s41598-023-35735-y. Sci Rep. 2023. PMID: 37353542 Free PMC article.
Cited by
-
Assessing the Association of Physician and Specialist Maldistribution with Out-of-hospital Cardiac Arrest Outcomes: Implications for Regulatory Policy.JMA J. 2025 Apr 28;8(2):506-516. doi: 10.31662/jmaj.2024-0241. Epub 2025 Feb 28. JMA J. 2025. PMID: 40416042 Free PMC article.
References
-
- Martin S.S., Aday A.W., Almarzooq Z.I., et al. 2024 heart disease and stroke statistics: a report of US and global data from the American heart association. Circulation. 2024;149:e347–e913. - PubMed
-
- Huebinger R., Vithalani V., Osborn L., et al. Community disparities in out of hospital cardiac arrest care and outcomes in Texas. Resuscitation. 2021;163:101–107. - PubMed
LinkOut - more resources
Full Text Sources
