

Predictive biomarkers for metachronous gastric cancer development after endoscopic resection of early gastric cancer
- PMID: 39171503
- PMCID: PMC11339598
- DOI: 10.1002/cam4.70104
Predictive biomarkers for metachronous gastric cancer development after endoscopic resection of early gastric cancer
Abstract
Objectives: We aimed to identify predictive markers for metachronous gastric cancer (MGC) in early gastric cancer (EGC) patients curatively treated with endoscopic submucosal dissection (ESD).
Materials and methods: From EGC patients who underwent ESD, bulk RNA sequencing was performed on non-cancerous gastric mucosa samples at the time of initial EGC diagnosis. This included 23 patients who developed MGC, and 23 control patients without additional gastric neoplasms for over 3 years (1:1 matched by age, sex, and Helicobacter pylori infection state). Candidate differentially-expressed genes were identified, from which biomarkers were selected using real-time quantitative polymerase chain reaction and cell viability assays using gastric cell lines. An independent validation cohort of 55 MGC patients and 125 controls was used for marker validation. We also examined the severity of gastric intestinal metaplasia, a known premalignant condition, at initial diagnosis.
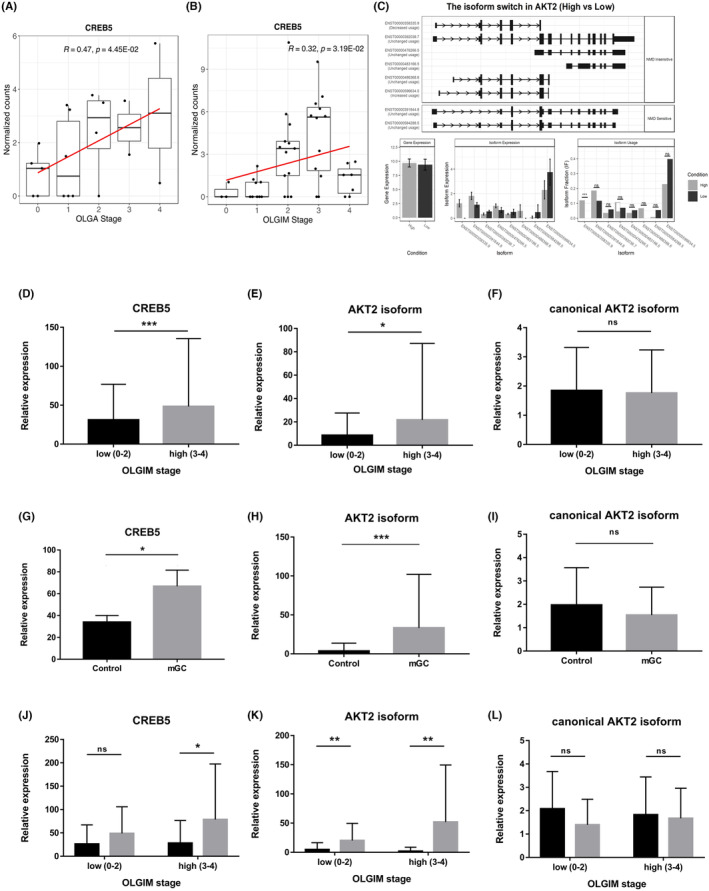
Results: From the discovery cohort, 86 candidate genes were identified of which KDF1 and CDK1 were selected as markers for MGC, which were confirmed in the validation cohort. CERB5 and AKT2 isoform were identified as markers related to intestinal metaplasia and were also highly expressed in MGC patients compared to controls (p < 0.01). Combining these markers with clinical data (age, sex, H. pylori and severity of intestinal metaplasia) yielded an area under the curve (AUC) of 0.91 (95% CI, 0.85-0.97) for MGC prediction.
Conclusion: Assessing biomarkers in non-cancerous gastric mucosa may be a useful method for predicting MGC in EGC patients and identifying patients with a higher risk of developing MGC, who can benefit from rigorous surveillance.
Keywords: RNA sequencing; biomarkers; endoscopic resection; gastric cancer; whole exome sequencing.
© 2024 The Author(s). Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures




References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394‐424. - PubMed
-
- Nakajima T, Oda I, Gotoda T, et al. Metachronous gastric cancers after endoscopic resection: how effective is annual endoscopic surveillance? Gastric Cancer. 2006;9(2):93‐98. - PubMed
-
- Min BH, Kim ER, Kim KM, et al. Surveillance strategy based on the incidence and patterns of recurrence after curative endoscopic submucosal dissection for early gastric cancer. Endoscopy. 2015;47(9):784‐793. - PubMed
-
- Hahn KY, Park JC, Kim EH, et al. Incidence and impact of scheduled endoscopic surveillance on recurrence after curative endoscopic resection for early gastric cancer. Gastrointest Endosc. 2016;84(4):628‐638 e1. - PubMed
MeSH terms
Substances
Grants and funding
- #NRF-2022R1A2B5B01001430/The National Research Foundation of Korea
- #NRF-2022R1A4A2000827/The National Research Foundation of Korea
- KCHUGR - 202002001/The Korean College of Helicobacter and Upper Gastrointestinal Research Foundation
- KCHUGR-202102001/The Korean College of Helicobacter and Upper Gastrointestinal Research Foundation
- #03-2020-0370/SNUH research fund
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
