

Trajectories of behavior and social cognition in behavioral variant frontotemporal dementia and primary psychiatric disorders: A call for better operationalization of socioemotional changes
- PMID: 39171655
- PMCID: PMC11555130
- DOI: 10.1111/ene.16426
Trajectories of behavior and social cognition in behavioral variant frontotemporal dementia and primary psychiatric disorders: A call for better operationalization of socioemotional changes
Abstract
Background and purpose: Behavioral variant frontotemporal dementia (bvFTD) and primary psychiatric disorders (PPD), such as mood, psychotic, and autism spectrum disorders, share similar clinical characteristics of behavior and social cognition. Better understanding of clinical progression in bvFTD and PPD is essential for adequate disease monitoring and trial design.
Methods: In this longitudinal study (N = 89), patients with bvFTD and PPD with at least one follow-up assessment were included from the Social Brain Project of the Alzheimer Center Amsterdam. Behavioral change and social cognitive decline were assessed via informant-rated questionnaires (Cambridge Behavioral Inventory-Revised, Frontal Behavioral Inventory [FBI], Stereotypy Rating Inventory, Frontotemporal Dementia Rating Scale, Revised Self-Monitoring Scale [RSMS]-caregiver) and patient assessment (Ekman 60-Faces Test, RSMS-patient, Emotional Contagion Scale). Clinical trajectories (median = 1.4 years, interquartile range = 1.0-2.2) were examined using linear mixed models. In a subsample, associations with baseline serum neurofilament light (sNfL) were examined.
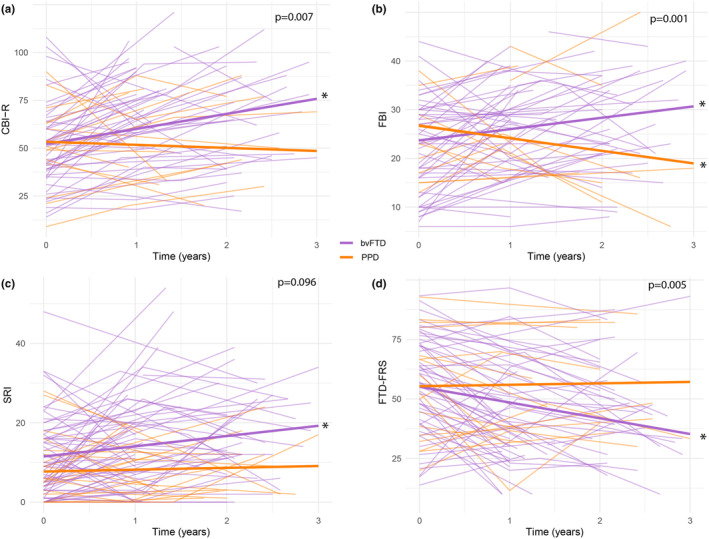
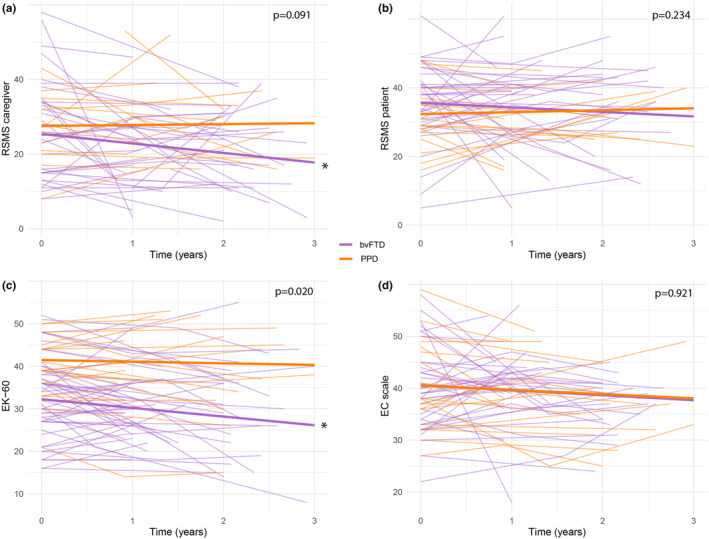
Results: At baseline, behavioral and social cognitive symptoms were similar between diagnosis groups, except for poorer emotion recognition in bvFTD. Over time, behavioral symptoms worsened in bvFTD, whereas most measures remained stable and the FBI improved in PPD. Regarding social cognition, emotion recognition and caregiver-reported socioemotional sensitivity worsened in bvFTD and remained stable in PPD. Patient-reported social cognitive measures did not change over time. Higher sNfL was associated with faster behavioral change.
Conclusions: Trajectories of behavior and social cognition differentiate bvFTD from PPD, provided that social cognition is not patient-reported. Therefore, we stress the need to optimize longitudinal social cognitive assessment in bvFTD. sNfL may be a useful prognostic marker of behavioral progression in neuropsychiatric populations.
Keywords: cohort study; disease progression; neuropsychiatric symptoms; outcome measures; social functioning.
© 2024 The Author(s). European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
The authors report no potential conflict of interest.
Figures
References
-
- Pose M, Cetkovich M, Gleichgerrcht E, Ibáñez A, Torralva T, Manes F. The overlap of symptomatic dimensions between frontotemporal dementia and several psychiatric disorders that appear in late adulthood. Int Rev Psychiatry. 2013;25(2):159‐167. - PubMed
-
- Gossink F, Schouws S, Krudop W, et al. Social cognition differentiates behavioral variant frontotemporal dementia from other neurodegenerative diseases and psychiatric disorders. Am J Geriatr Psychiatry. 2018;26(5):1545‐7214. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
