

Timing of Influenza Antiviral Therapy and Risk of Death in Adults Hospitalized With Influenza-Associated Pneumonia, Influenza Hospitalization Surveillance Network (FluSurv-NET), 2012-2019
- PMID: 39172994
- PMCID: PMC11847407
- DOI: 10.1093/cid/ciae427
Timing of Influenza Antiviral Therapy and Risk of Death in Adults Hospitalized With Influenza-Associated Pneumonia, Influenza Hospitalization Surveillance Network (FluSurv-NET), 2012-2019
Abstract
Background: Pneumonia is common in adults hospitalized with laboratory-confirmed influenza, but the association between timeliness of influenza antiviral treatment and severe clinical outcomes in patients with influenza-associated pneumonia is not well characterized.
Methods: We included adults aged ≥18 years hospitalized with laboratory-confirmed influenza and a discharge diagnosis of pneumonia over 7 influenza seasons (2012-2019) sampled from a multistate population-based surveillance network. We evaluated 3 treatment groups based on timing of influenza antiviral initiation relative to admission date (day 0, day 1, days 2-5). Baseline characteristics and clinical outcomes were compared across groups using unweighted counts and weighted percentages accounting for the complex survey design. Logistic regression models were generated to evaluate the association between delayed treatment and 30-day all-cause mortality.
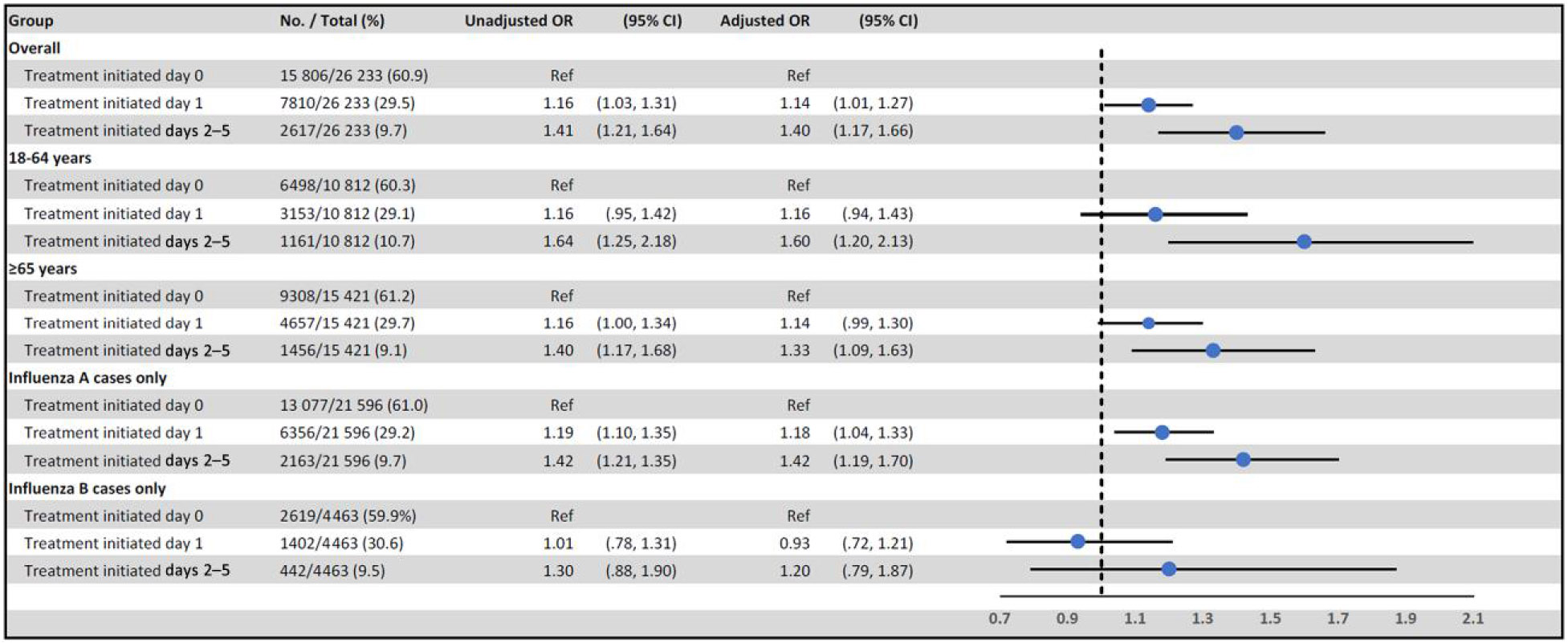
Results: A total of 26 233 adults were sampled in the analysis. Median age was 71 years and most (92.2%) had ≥1 non-immunocompromising condition. Overall, 60.9% started antiviral treatment on day 0, 29.5% on day 1, and 9.7% on days 2-5 (median, 2 days). Baseline characteristics were similar across groups. Thirty-day mortality occurred in 7.5%, 8.5%, and 10.2% of patients who started treatment on day 0, day 1, and days 2-5, respectively. Compared to those treated on day 0, adjusted odds ratio for death was 1.14 (95% confidence interval [CI], 1.01-1.27) in those starting treatment on day 1 and 1.40 (95% CI, 1.17-1.66) in those starting on days 2-5.
Conclusions: Delayed initiation of antiviral treatment in patients hospitalized with influenza-associated pneumonia was associated with higher risk of death, highlighting the importance of timely initiation of antiviral treatment at admission.
Keywords: antiviral; hospitalization; influenza; mortality; oseltamivir.
Published by Oxford University Press on behalf of Infectious Diseases Society of America 2024.
Conflict of interest statement
Potential conflicts of interest. K. Y.-H., J. M., I. A., and W. S. report grants from the CDC, during the conduct of the study. A. F. and L. R. report grants from the Michigan Department of Health and Human Services, during the conduct of the study. M. L. M. reports grants from the CDC Emerging Infections Program, during the conduct of the study. R. L. reports grants from the CDC Emerging Infections Program cooperative agreement, during the conduct of the study, and fee for work as Associate Editor for the American Academy of Pediatrics Report of the Committee on Infectious Diseases (Red Book), which donated to the Minnesota Department of Health. H. K. T. reports funding from CDC for this work and other areas of research. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Centers for Disease Control and Prevention. Past seasons estimated influenza disease burden averted by vaccination. 2024. Available at: https://www.cdc.gov/flu/vaccines-work/past-burden-averted-est.html. Accessed 16 October 2023.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
