

Review
doi: 10.1007/s00393-024-01560-5.
Epub 2024 Aug 22.
Castleman's disease in the rheumatological practice
Affiliations
- PMID: 39174716
- PMCID: PMC11655606
- DOI: 10.1007/s00393-024-01560-5
Item in Clipboard
Review
Castleman's disease in the rheumatological practice
Z Rheumatol.
2024 Dec.
No abstract available
Conflict of interest statement
Declarations. Conflict of interest: M. Schmalzing, O. Sander, M. Seidl, R. Marks, N. Blank, I. Kötter, M. Tiemann, M. Backhaus, B. Manger, K. Hübel, U. Müller-Ladner, and J. Henes declare the following conflict of interest: consulting and lecturing activities for EUSA-Pharma. U. Müller-Ladner and M. Backhaus declare that there is no conflict of interest. For this article no studies with human participants or animals were performed by any of the authors. All studies mentioned were in accordance with the ethical standards indicated in each case. The supplement containing this article is not sponsored by industry.
Figures
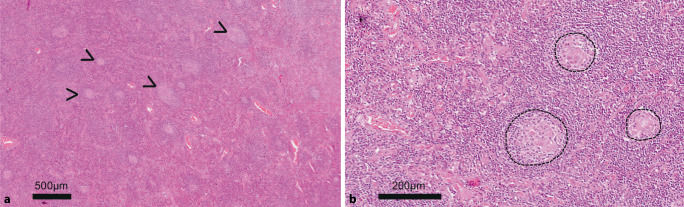
Histology for case report 1 (5× and 20× magnification for a and b, respectively). a Overview magnification of the axillary lymph node with secondary lymphofollicular hyperplasia (secondary follicles marked by an arrowhead as an example). The overall very small secondary follicles are striking. b Regressive, hyalinized germinal centers (dashed line) with an at least partially layered mantle zone (germinal center bottom left)

Histology for case report 2 (5×, 40×, 10×, 20× magnification for a–c and d, respectively). a Overview magnification of the mediastinal lymph node with preserved compartments (follicles are exemplarily marked by an arrowhead; left is without and right is with a germinal center). b Typical “lollipop” pattern of the hyaline vascular transformed regressive germinal center (k) due to the prominent vessel (g) and the onion skin-like structured mantle zone (m); adjacent to this, perisinusoidal/perivenular increased plasma cells (pc). c Condensed follicular dendritic cells within the germinal centers, d with an overall significantly increased plasma cell count; there are also increased IgG 4-positive plasma cells, but without eosinophilia, fibrosis, or obliterative phlebitis, thus histologically atypical for IgG 4-associated disease. The proliferation of plasma cells is indicated serologically by hypergammaglobulinemia

Clinical classification of Castleman’s disease according to lymph node involvement and clinical presentation (modified according to [3])
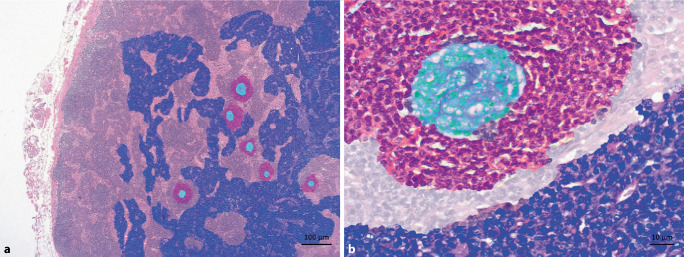
False-color imaging for case report 2. a Overview magnification to highlight the clear plasma cell proliferation (shown in purple; turquoise germinal centers, magenta mantle zone). b Higher magnification: plasma cell location is physiologically perisinusoidal/perivenular. Afferent lymphatic vessels drain into the lymph node sinuses, i.e., antigens arriving from the periphery first come into contact with antibodies of the already established plasma cells. Class-switched plasma cells, in turn, originate from the germinal center response (turquoise) as a selection outcome in competition for the antigen, which is stored on follicular dendritic cells (FDC) in the germinal center in an immune complex-bound manner (higher-affinity antibodies displace lower-affinity ones in the course of the immune response). Naive and memory B cells of the mantle zone (magenta) may enter the germinal center response

Schematically simplified presentation of the germinal center reaction. Ab antibodies, DC dendritic cell, FDC follicular DC, GC germinal center, MBC memory B cells, PC antibody-producing long-lived plasma cells
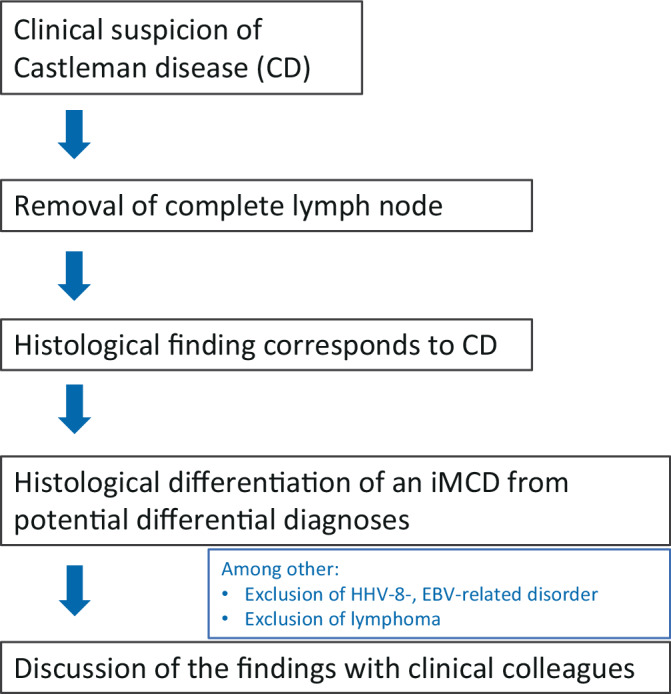
In case of clinical suspicion of Castleman’s disease: procedure from the pathologist’s point of view
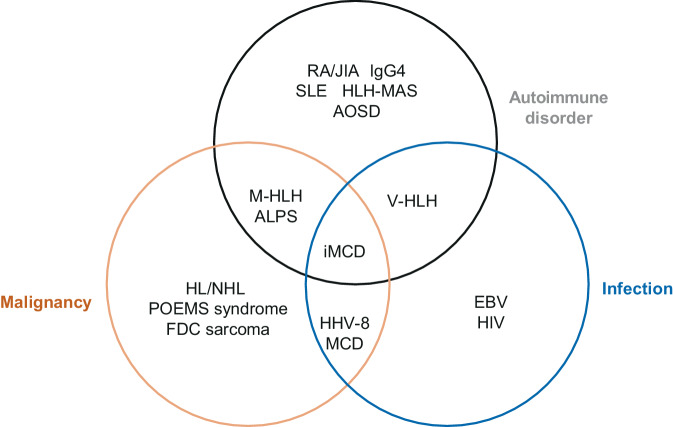
Spectrum of possible differential diagnoses of autoimmune, malignant, and infection-related diseases in iMCD. ALPS autoimmune lymphoproliferative syndrome; AOSD adult-onset Still’s disease; EBV Epstein–Barr virus; FDC follicular dendritic cell; HHV‑8 human herpesvirus 8; HLH hemophagocytic lymphohistiocytosis; M‑HLH malignancy-associated HLH; V‑HLH virus-associated HLH; HLH-MAS HLH macrophage activation syndrome; POEMS polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, skin lesions; RA rheumatoid arthritis; JIA juvenile idiopathic arthritis; SLE systemic lupus erythematosus (according to Fajgenbaum et al. [3])
References
-
- Castleman B (1954) CASE records of the Massachusetts general hospital weekly clinicopathological exercises: case 40011. N Engl J Med 250:26–30 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
