

A dosimetric comparison of brachytherapy sources for endometrial cancer: an electronic brachytherapy and an iridium-192 source with multichannel cylinders and a three-dimensional technique
- PMID: 39174903
- PMCID: PMC11342593
- DOI: 10.1186/s12885-024-12814-5
A dosimetric comparison of brachytherapy sources for endometrial cancer: an electronic brachytherapy and an iridium-192 source with multichannel cylinders and a three-dimensional technique
Abstract
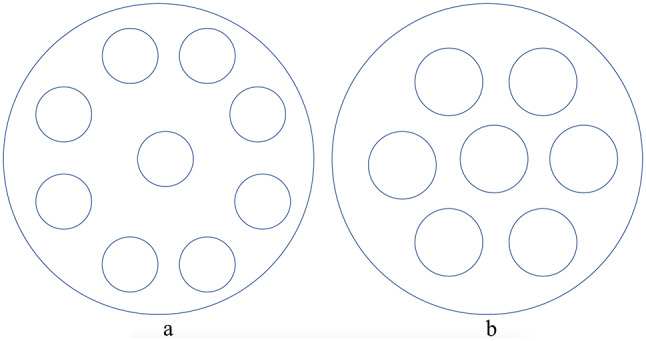
Background and purpose: Ir192 vaginal brachytherapy (IBT) is commonly used for patients with postoperative endometrial cancer (EC). We devised a novel multichannel vaginal applicator that could be equipped with an electronic brachytherapy (EBT) device. We aimed to explore the differences in physical parameters between the EBT and IBT.
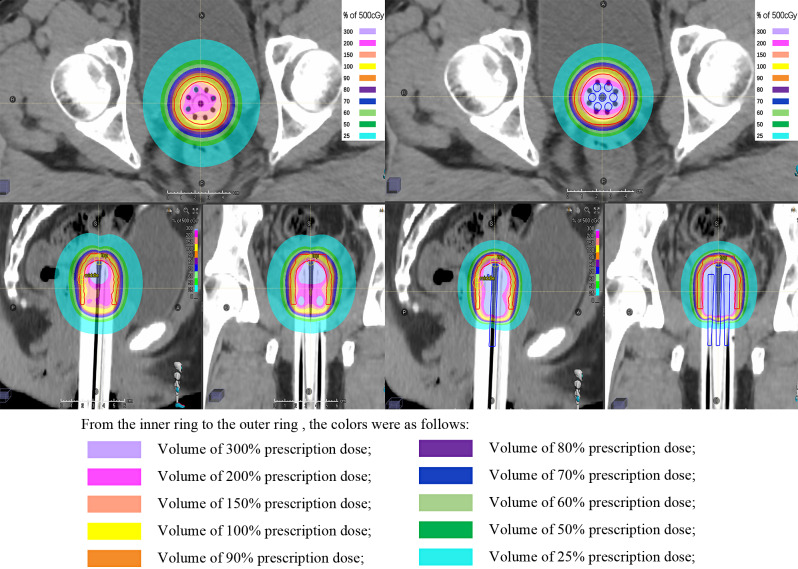
Materials and methods: This retrospective study included 20 EC patients who received adjuvant IBT from March 1, 2023, to May 1, 2023. Multichannel vaginal cylinders were used, and three-dimensional plans were generated. We designed an electronic multichannel vaginal applicator model and simulated a three-dimensional EBT plan. In order to ensure comparability, D90 of the CTV for the EBT plan was normalized to be equivalent to that of the IBT plan for the same patient.
Results: Twenty EBT plans were compared with 20 IBT plans. Results showed, the mean D90 value of clinical target volume (CTV) was 536.1 cGy for both treatment plans. For the mean dose of CTV, the EBT was significantly greater (738.3 vs. 684.3 cGy, p = 0.000). There was no significant difference in CTV coverage between the EBT and IBT plans. For high-dose areas (V200% and V150%), the EBTs were significantly greater. There were no significant differences in the maximum doses to the vaginal mucosa between the EBT and IBT, whether at the apex or in the middle segment. For the bladder and rectum, both the low-dose area and high-dose area were significantly lower in the EBT plans. For the conformity index, there was no significant difference between the EBT and IBT plans. For the dose homogeneity index, the EBT value was lower.
Conclusion: In conclusion, under the premise of a three-dimensional brachytherapy plan, for patients receiving multichannel vaginal applicator brachytherapy, compared with IBT, EBT could reduce the dose to the surrounding organs at risk while maintaining the dose in the target area.
Keywords: Electronic brachytherapy; Iridium-192 brachytherapy; Multichannel vaginal applicator; Physical parameters.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
