

Predicting tumor invasion depth in gastric cancer: developing and validating multivariate models incorporating preoperative IVIM-DWI parameters and MRI morphological characteristics
- PMID: 39175075
- PMCID: PMC11340138
- DOI: 10.1186/s40001-024-02017-w
Predicting tumor invasion depth in gastric cancer: developing and validating multivariate models incorporating preoperative IVIM-DWI parameters and MRI morphological characteristics
Abstract
Introduction: Accurate assessment of the depth of tumor invasion in gastric cancer (GC) is vital for the selection of suitable patients for neoadjuvant chemotherapy (NAC). Current problem is that preoperative differentiation between T1-2 and T3-4 stage cases in GC is always highly challenging for radiologists.
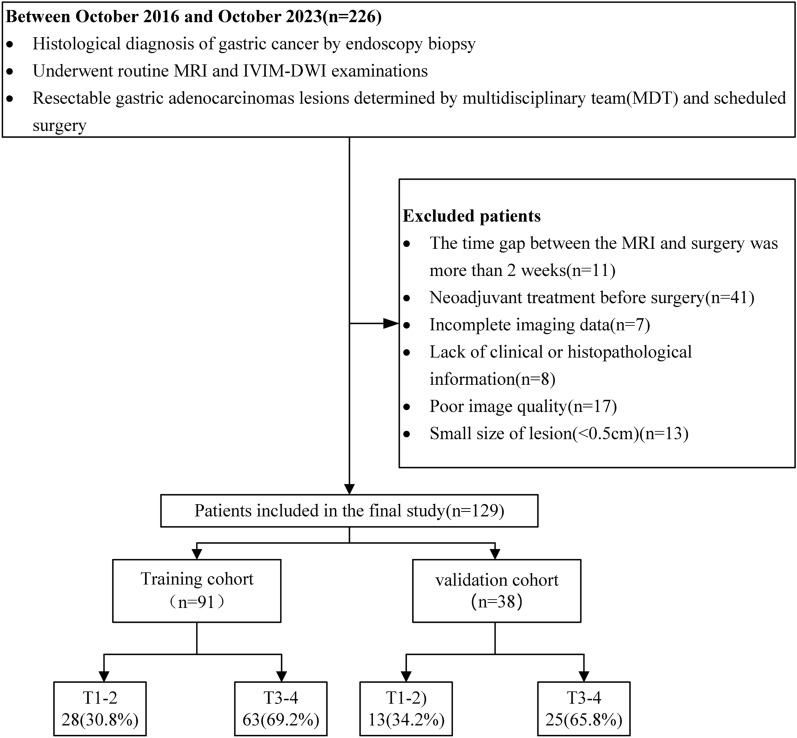
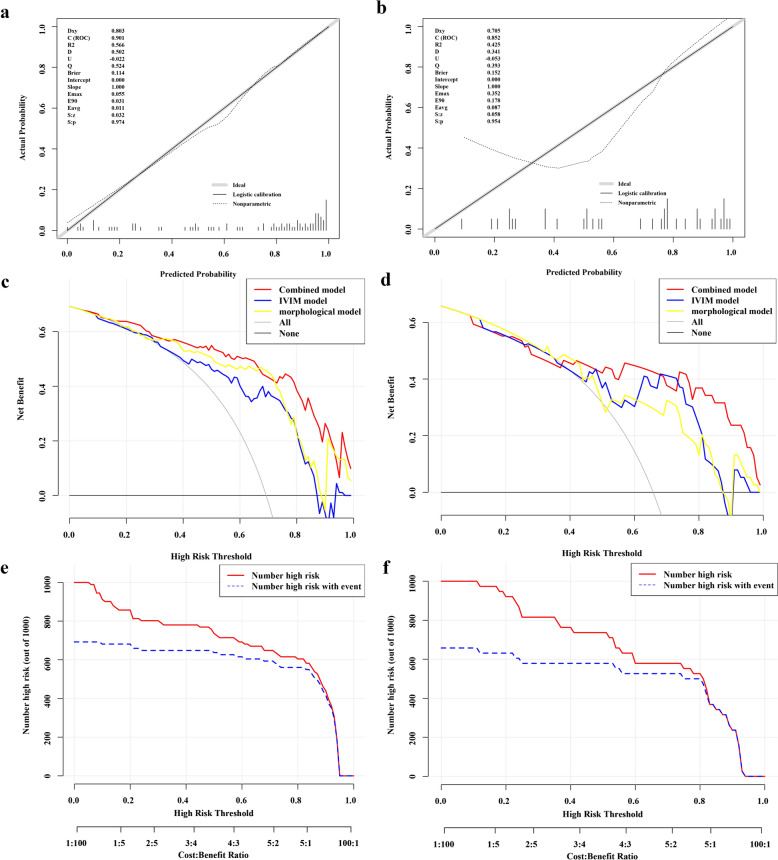
Methods: A total of 129 GC patients were divided into training (91 cases) and validation (38 cases) cohorts. Pathology from surgical specimens categorized patients into T1-2 and T3-4 stages. IVIM-DWI and MRI morphological characteristics were evaluated, and a multimodal nomogram was developed. The MRI morphological model, IVIM-DWI model, and combined model were constructed using logistic regression. Their effectiveness was assessed using receiver operating characteristic (ROC) curves, calibration curves, decision curve analysis (DCA), and clinical impact curves (CIC).
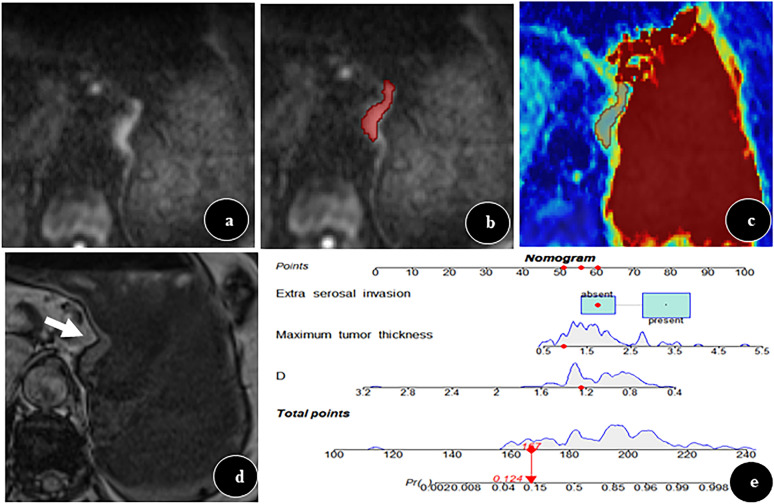
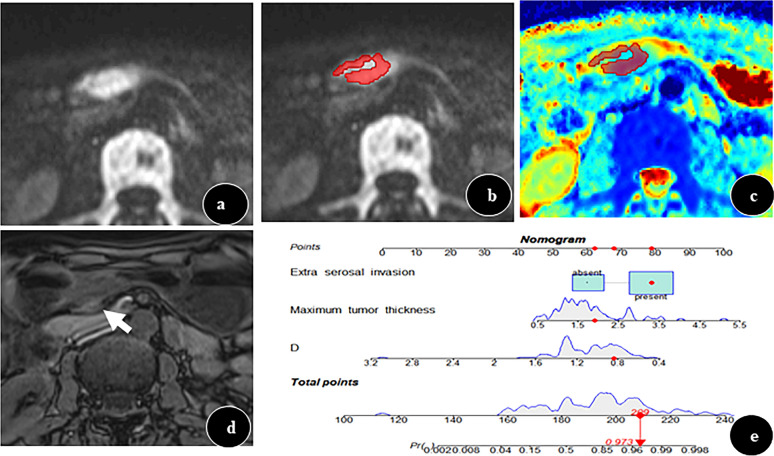
Results: The combined nomogram, integrating preoperative IVIM-DWI parameters (D value) and MRI morphological characteristics (maximum tumor thickness, extra-serosal invasion), achieved the highest area under the curve (AUC) values of 0.901 and 0.883 in the training and validation cohorts, respectively. No significant difference was observed between the AUCs of the IVIM-DWI and MRI morphological models in either cohort (training: 0.796 vs. 0.835, p = 0.593; validation: 0.794 vs. 0.766, p = 0.79).
Conclusion: The multimodal nomogram, combining IVIM-DWI parameters and MRI morphological characteristics, emerges as a promising tool for assessing tumor invasion depth in GC, potentially guiding the selection of suitable candidates for neoadjuvant chemotherapy (NAC) treatment.
Keywords: Diffusion weighted imaging; Intravoxel incoherent motion; Neoplasm staging; Nomogram; Stomach neoplasms.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Global cancer statistics, et al. GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2020. 10.3322/caac.21660. 10.3322/caac.21660 - DOI
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
