

Patient-Related Factors Associated With Long-Term Outcomes After Successful Endoscopic Balloon Dilation For Crohn's Disease-Associated Ileo-Colic Strictures: A Systematic Review and Meta-analysis
- PMID: 39175792
- PMCID: PMC11339545
- DOI: 10.1093/crocol/otae041
Patient-Related Factors Associated With Long-Term Outcomes After Successful Endoscopic Balloon Dilation For Crohn's Disease-Associated Ileo-Colic Strictures: A Systematic Review and Meta-analysis
Abstract
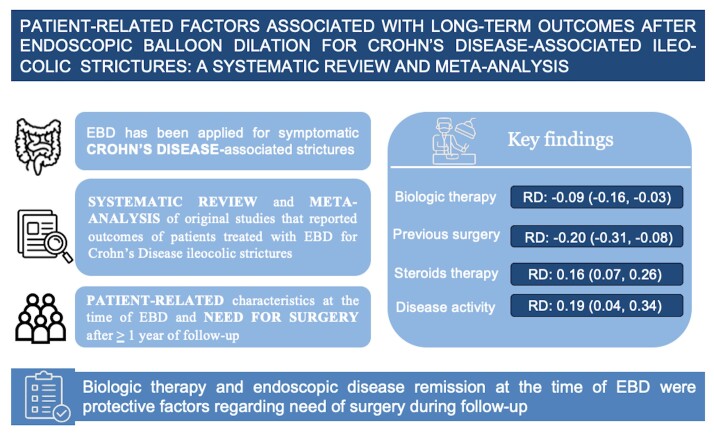
Background: Successful Crohn's disease (CD) therapy relies on timely and precise management strategies. Endoscopic balloon dilation (EBD) has been applied as a first-line treatment for symptomatic CD-associated strictures due to its minimally invasive nature and the possibility of preserving intestinal length.
Objective: The aim of the present study was to determine patient-related predictive factors associated with the need for surgery for CD-associated ileocolic strictures after technically successful EBD.
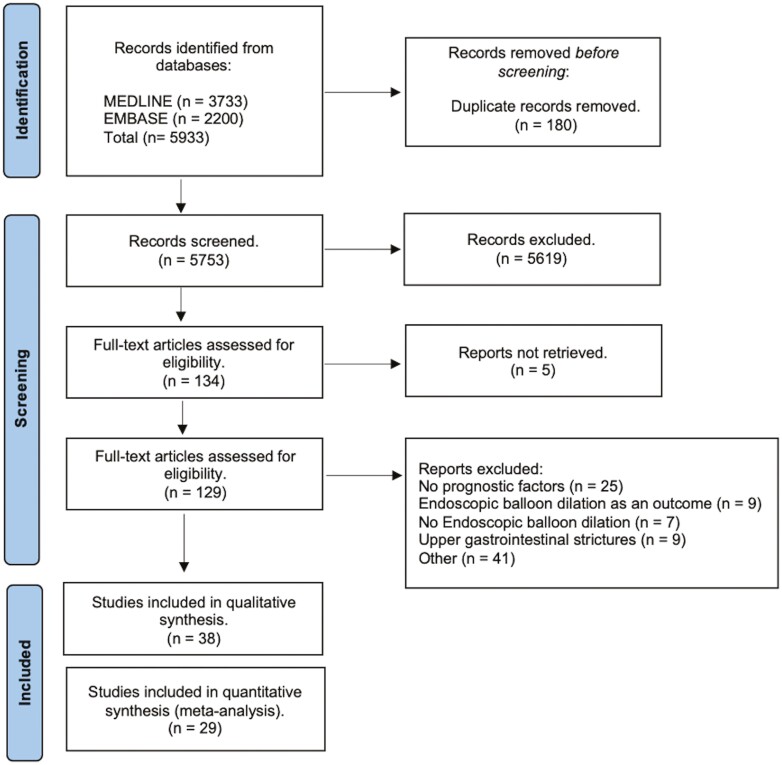
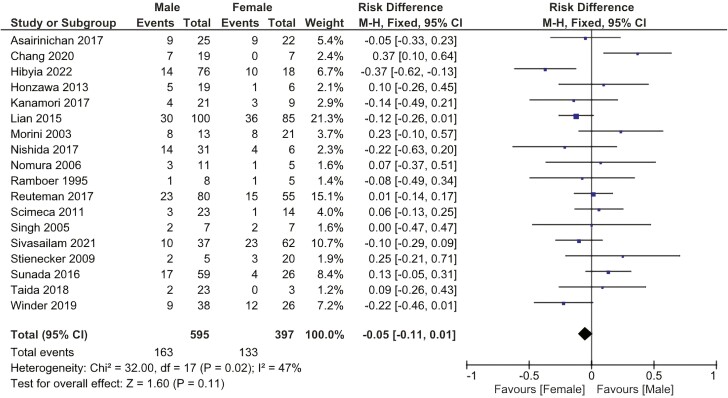
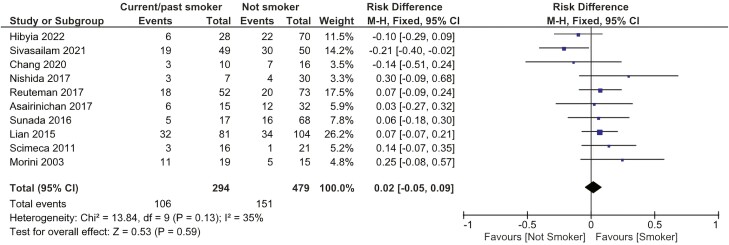
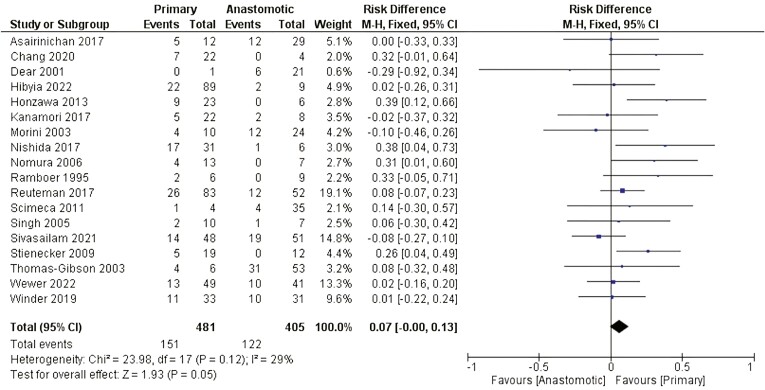
Methods: All original studies published before December 2023 that reported the outcomes of patients treated with EBD for ileocolic strictures secondary to CD and described follow-up for at least 1 year were included. The difference in risk of needing surgery was calculated for 8 different patient characteristics (Sex, smoking habit, previous surgery, biologic therapy, steroids, immunosuppressors, nature of the stricture, and endoscopic disease activity).
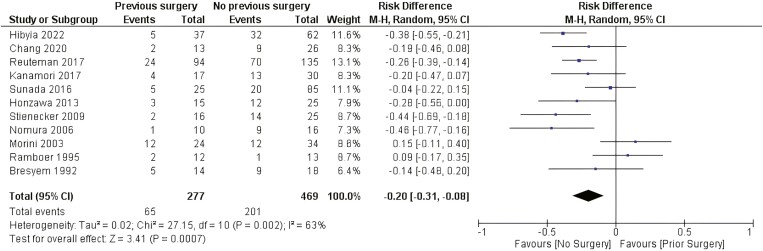
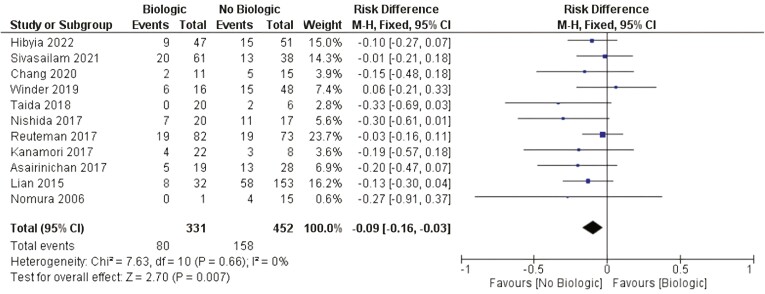
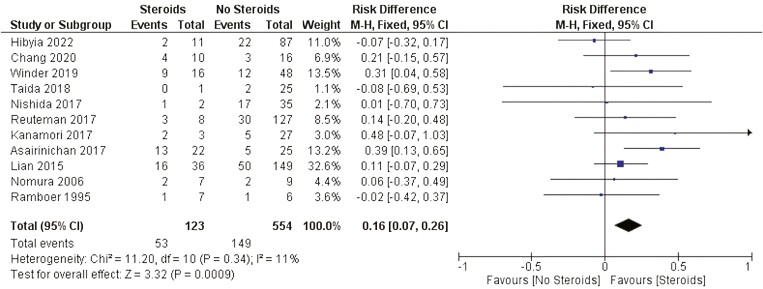
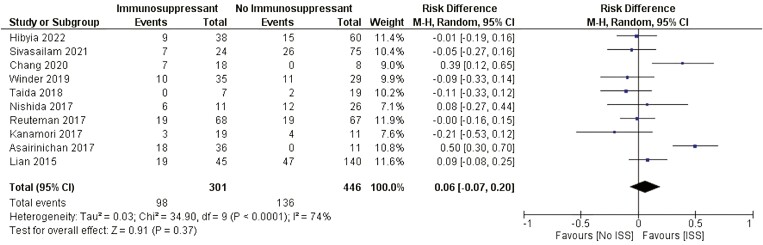
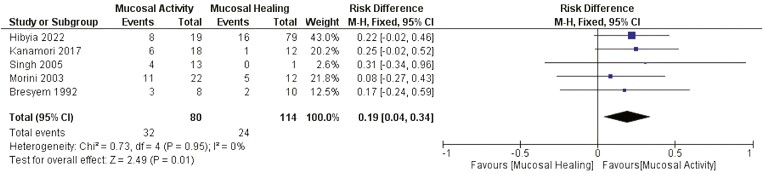
Results: There were significant differences in the risk of needing surgery after EBD among patients who underwent surgery and patients without a history of surgery (RD: -0.20 [-0.31, -0.08]), patients with endoscopic mucosal activity and patients in remission at the time of EBD (RD: 0.19 [0.04, 0.34]), patients using biologics at the time of EBD and patients not using biologics (RD: -0.09 [-0.16, -0.03]), and patients using steroids and those not using steroids at the time of EBD (RD: 0.16 [0.07, 0.26]).
Conclusions: The use of biologics and endoscopic disease remission at the time of EBD were protective factors against the need for surgery. No previous surgery or use of steroids at the time of EBD was associated with the need for surgery during follow-up.
Keywords: Crohn’s disease; endoscopic balloon dilation; strictures.
© The Author(s) 2024. Published by Oxford University Press on behalf of Crohn's & Colitis Foundation.
Conflict of interest statement
None declared. Competing interests: The authors declare that they have no conflicts of interest.
Figures

References
-
- GBD 2017 Inflammatory Bowel Disease Collaborators. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020;5(1):17-30. doi: 10.1016/S2468-1253(19)30333-4 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous