

Case Report: Plummer's adenoma in Prader-Willi syndrome
- PMID: 39175805
- PMCID: PMC11338776
- DOI: 10.3389/fped.2024.1388437
Case Report: Plummer's adenoma in Prader-Willi syndrome
Abstract
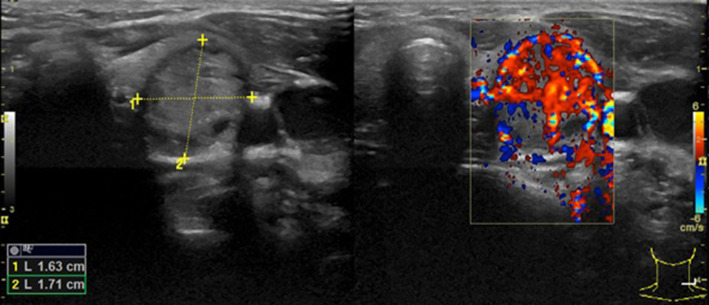
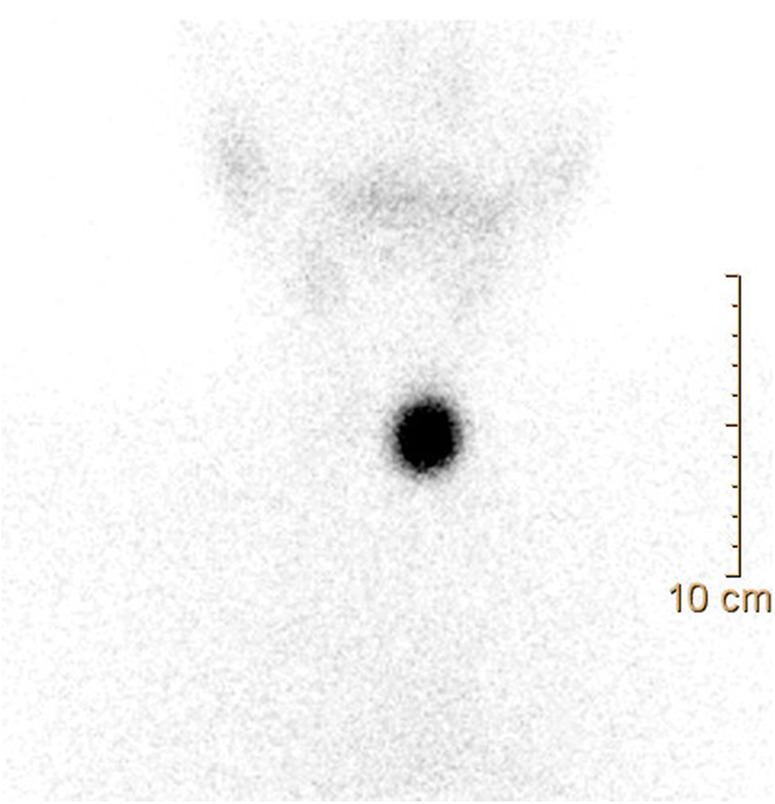
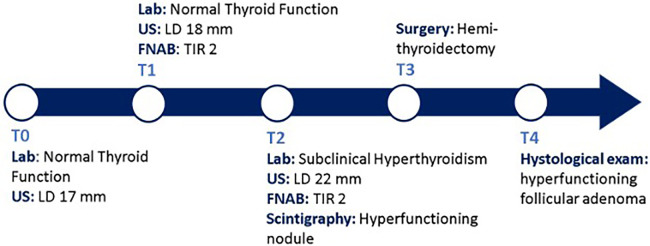
Thyroid nodules in children are less common than in adults but they are approximately two- to three-fold more likely to be malignant in children. Among thyroid nodular diseases, Plummer's adenoma occurs very rarely in pediatrics, and currently, there is no literature providing evidence of this diagnosis in patients with Prader-Willi syndrome (PWS). We report the case of a 9-year-old Caucasian boy affected by PWS presenting with a rapidly growing palpable mass in the thyroid lodge associated with subclinical hyperthyroidism. Laboratory and other examinations (thyroid ultrasound, fine-needle aspiration of the nodule, and scintigraphy) were strongly suggestive for Plummer's adenoma; therefore, the patient underwent left hemithyroidectomy surgery, and anatomo-pathological examination confirmed the diagnosis. Our case describes the first evidence of an isolated follicular adenoma in children with PWS. Surgery is the only therapeutic option in younger children. Further evidence is needed to assess the possible correlation between these two conditions and the existence of potential risk factors.
Keywords: GH therapy; Plummer’s adenoma; children; subclinical hyperthyroidism; thyroid nodule.
© 2024 Corica, Toscano, Moleti, Pepe, Campenni, Fadda, Dionigi, Romeo, Aversa and Wasniewska.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors declared that they were an editorial board member of Frontiers at the time of submission. This had no impact on the peer review process and final decision.
Figures
References
-
- Shimura H, Sobue T, Takahashi H, Yasumura S, Ohira T, Ohtsuru A, et al. Thyroid examination unit of the radiation medical center for the Fukushima Health Management Survey Group. Findings of thyroid ultrasound examination within 3 years after the Fukushima nuclear power plant accident: the Fukushima health management survey. J Clin Endocrinol Metab. (2018) 103(3):861–9. 10.1210/jc.2017-01603 - DOI - PubMed