

Immediate inferior alveolar nerve reconstruction: Improving warfighter quality of life following mandibulectomy or traumatic avulsion of the mandible
- PMID: 39177612
- PMCID: PMC11613050
- DOI: 10.3233/NRE-230253
Immediate inferior alveolar nerve reconstruction: Improving warfighter quality of life following mandibulectomy or traumatic avulsion of the mandible
Abstract
Background: Mandibular reconstruction has historically been challenging due to the complex, highly functional, and esthetic nature of the anatomy. The most common etiologies of these defects requiring resection include trauma, benign tumors, and malignant pathology. Mandibular defects have been treated with little consideration for neural reconstruction, leaving patient's orally incompetent with associated social stigma. Although recent advances in reconstructive techniques improve oral rehabilitation, immediate inferior alveolar nerve (IAN) reconstruction has not been widely adapted.
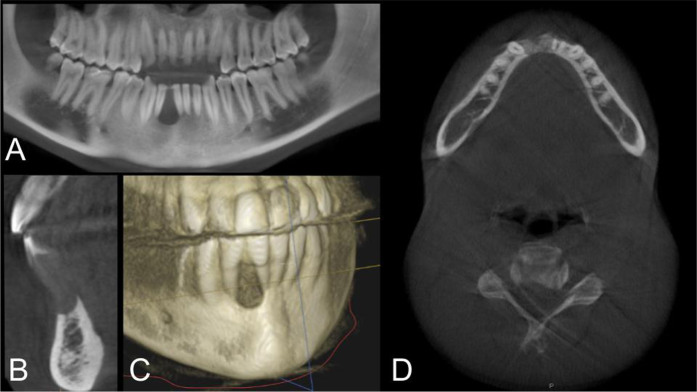
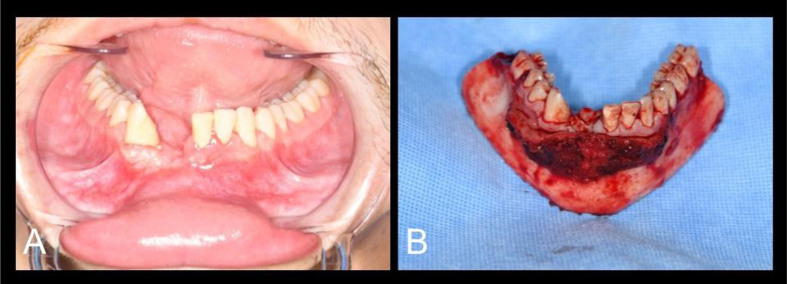
Objective: Here-in we seek to discuss the innovations of neural reconstruction of large segment mandibular defects and associated IAN defects and present an example case performed at Naval Medical Center San Diego (NMCSD).
Methods: Pertinent literature discussing maxillofacial reconstruction and nerve repair using autogenous nerve harvest and allograft was queried from available online resources.
Results: Six patients have received immediate reconstruction of the IAN using processed nerve allograft over the past three years. All obtained sensation to S3 within six months of surgery.
Conclusion: IAN repair using nerve allografts in conjunction with free flap reconstruction for large mandibular defects is a viable treatment and should be the new paradigm in maxillofacial reconstruction as it provides substantial quantifiable and qualitative improvements in social, functional, and esthetic outcomes of care.
Keywords: Fibula free flap; inferior alveolar nerve; jaw-in-a-day; maxillofacial reconstruction; nerve allograft.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures



Similar articles
-
Outcomes of Immediate Allograft Reconstruction of Long-Span Defects of the Inferior Alveolar Nerve.J Oral Maxillofac Surg. 2016 Dec;74(12):2507-2514. doi: 10.1016/j.joms.2016.05.029. Epub 2016 Jun 14. J Oral Maxillofac Surg. 2016. PMID: 27376182
-
Inferior alveolar nerve reconstruction in extensive mandibular resection: Technical notes.J Plast Reconstr Aesthet Surg. 2021 Mar;74(3):634-636. doi: 10.1016/j.bjps.2020.11.040. Epub 2020 Dec 10. J Plast Reconstr Aesthet Surg. 2021. PMID: 33339753
-
Immediate Inferior Alveolar Nerve Reconstruction With Ablative Mandibular Resection Results in Functional Sensory Recovery.J Oral Maxillofac Surg. 2024 Jan;82(1):126-133. doi: 10.1016/j.joms.2023.09.025. Epub 2023 Oct 5. J Oral Maxillofac Surg. 2024. PMID: 37898153
-
Fibular Reconstruction of the Maxilla and Mandible with Immediate Implant-Supported Prosthetic Rehabilitation: Jaw in a Day.Oral Maxillofac Surg Clin North Am. 2019 Aug;31(3):369-386. doi: 10.1016/j.coms.2019.03.002. Epub 2019 Jun 1. Oral Maxillofac Surg Clin North Am. 2019. PMID: 31164268 Review.
-
Reconstructive Options for Inferior Alveolar and Lingual Nerve Injuries After Dental and Oral Surgery: An Evidence-Based Review.Ann Plast Surg. 2019 Jun;82(6):653-660. doi: 10.1097/SAP.0000000000001783. Ann Plast Surg. 2019. PMID: 30648997 Review.
References
-
- Chang, Y. M., Rodriguez, E. D., Chu, Y. M., Tsai, C. Y., Wei, F. C. (2012). Inferior alveolar nerve reconstruction with interpositional sural nerve graft: a sensible addition to one-stage mandibular reconstruction. J Plast Reconstr Aesthet Surg, 65(6), 757–762. 10.1016/j.bjps.2011.12.028. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
