

Comparative renal outcomes of matched cohorts of patients with type 2 diabetes receiving SGLT2 inhibitors or GLP-1 receptor agonists under routine care
- PMID: 39177691
- PMCID: PMC11519175
- DOI: 10.1007/s00125-024-06251-z
Comparative renal outcomes of matched cohorts of patients with type 2 diabetes receiving SGLT2 inhibitors or GLP-1 receptor agonists under routine care
Abstract
Aims/hypothesis: We compared the effects of sodium-glucose cotransporter 2 (SGLT2) inhibitors (SGLT2i) and glucagon-like peptide-1 receptor agonists (GLP-1RA) on renal outcomes in individuals with type 2 diabetes, focusing on the changes in eGFR and albuminuria.
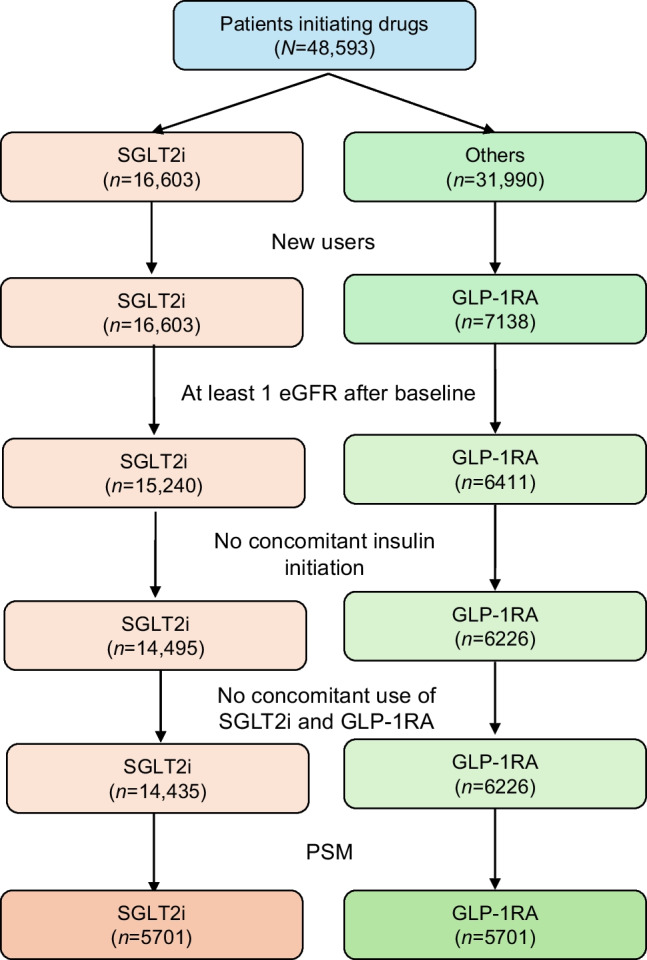
Methods: This was a multicentre retrospective observational study on new users of diabetes medications. Participant characteristics were assessed before and after propensity score matching. The primary endpoint, change in eGFR, was analysed using mixed-effects models. Secondary endpoints included categorical eGFR-based outcomes and changes in albuminuria. Subgroup and sensitivity analyses were performed to assess robustness of the findings.
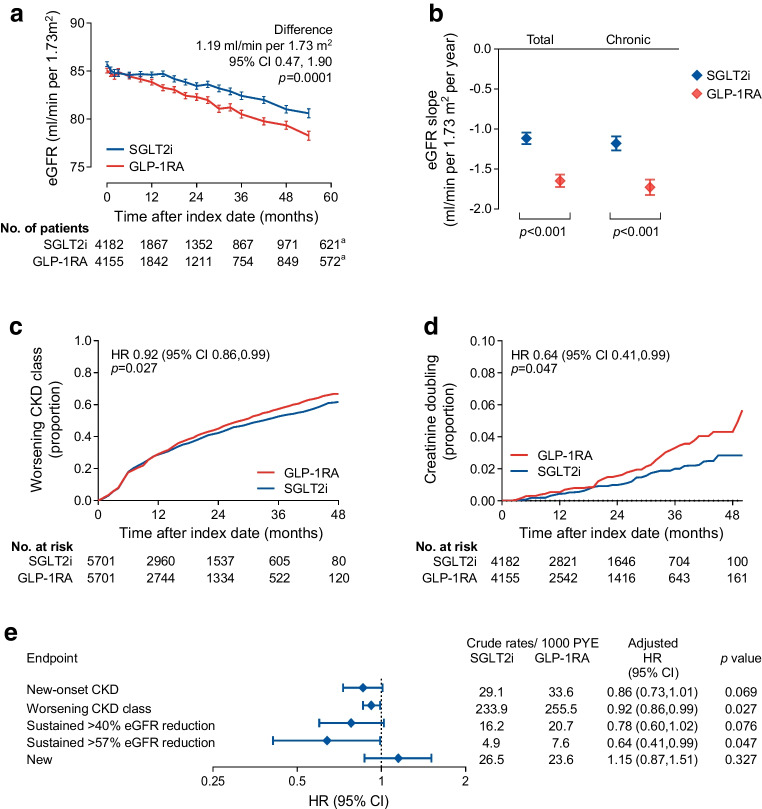
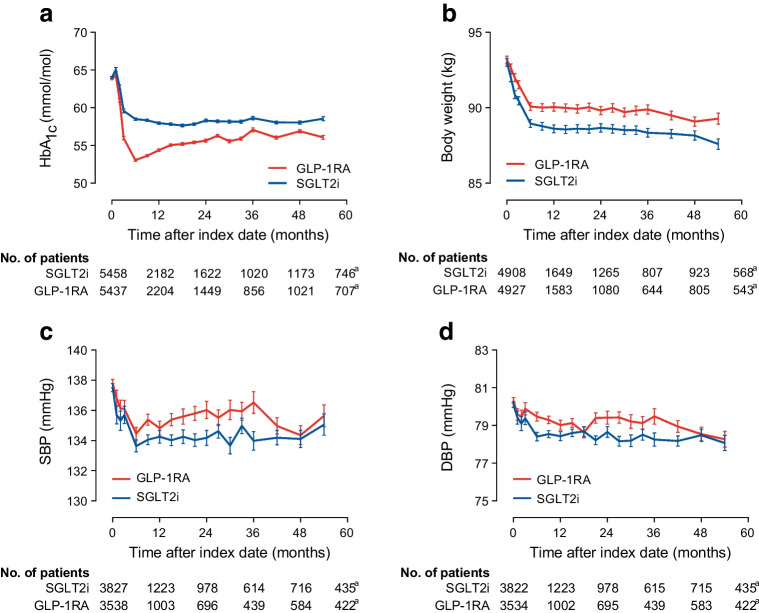
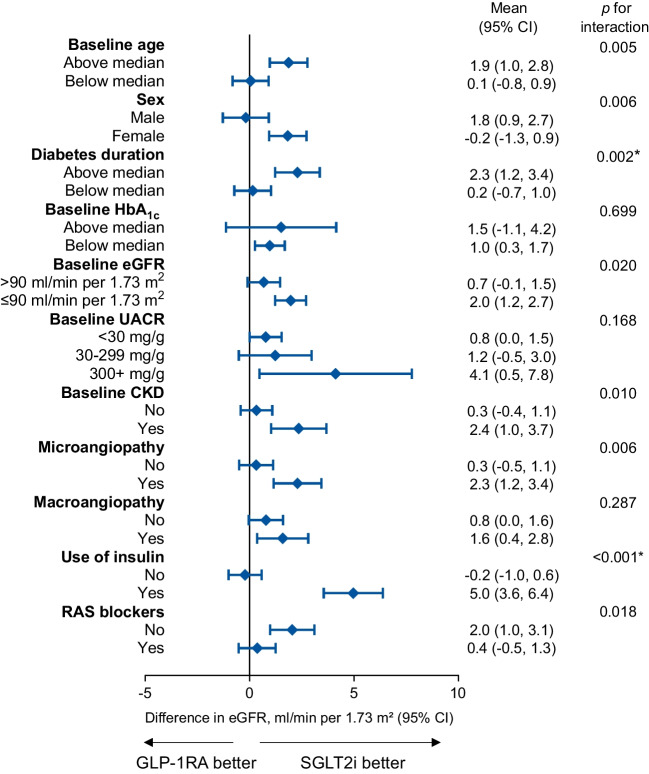
Results: After matching, 5701 participants/group were included. Participants were predominantly male, aged 61 years, with a 10 year duration of diabetes, a baseline HbA1c of 64 mmol/mol (8.0%) and BMI of 33 kg/m2. Chronic kidney disease (CKD) was present in 23% of participants. During a median of 2.1 years, from a baseline of 87 ml/min per 1.73 m2, eGFR remained higher in the SGLT2i group compared with the GLP-1RA group throughout the observation period by 1.2 ml/min per 1.73 m2. No differences were detected in albuminuria change. The SGLT2i group exhibited lower rates of worsening CKD class and favourable changes in BP compared with the GLP-1RA group, despite lesser HbA1c decline. SGLT2i also reduced eGFR decline better than GLP-1RA in participants without baseline CKD.
Conclusions/interpretation: In individuals with type 2 diabetes, treatment with SGLT2i was associated with better preservation of renal function compared with GLP-1RA, as evidenced by slower decline in eGFR. These findings reinforce SGLT2i as preferred agents for renal protection in this patient population.
Keywords: Kidney disease; Obesity; Pharmacoepidemiology; Real-world; Type 2 diabetes.
© 2024. The Author(s).
Figures
References
-
- Wang V, Vilme H, Maciejewski ML, Boulware LE (2016) The economic burden of chronic kidney disease and end-stage renal disease. Semin Nephrol 36(4):319–330. 10.1016/j.semnephrol.2016.05.008 - PubMed
-
- Fioretto P, Pontremoli R (2022) Expanding the therapy options for diabetic kidney disease. Nat Rev Nephrol 18(2):78–79. 10.1038/s41581-021-00522-3 - PubMed
-
- Mosenzon O, Wiviott SD, Cahn A et al (2019) Effects of dapagliflozin on development and progression of kidney disease in patients with type 2 diabetes: an analysis from the DECLARE-TIMI 58 randomised trial. Lancet Diabetes Endocrinol 7(8):606–617. 10.1016/S2213-8587(19)30180-9 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
