

AI-Driven Diagnostic Assistance in Medical Inquiry: Reinforcement Learning Algorithm Development and Validation
- PMID: 39178403
- PMCID: PMC11380057
- DOI: 10.2196/54616
AI-Driven Diagnostic Assistance in Medical Inquiry: Reinforcement Learning Algorithm Development and Validation
Abstract
Background: For medical diagnosis, clinicians typically begin with a patient's chief concerns, followed by questions about symptoms and medical history, physical examinations, and requests for necessary auxiliary examinations to gather comprehensive medical information. This complex medical investigation process has yet to be modeled by existing artificial intelligence (AI) methodologies.
Objective: The aim of this study was to develop an AI-driven medical inquiry assistant for clinical diagnosis that provides inquiry recommendations by simulating clinicians' medical investigating logic via reinforcement learning.
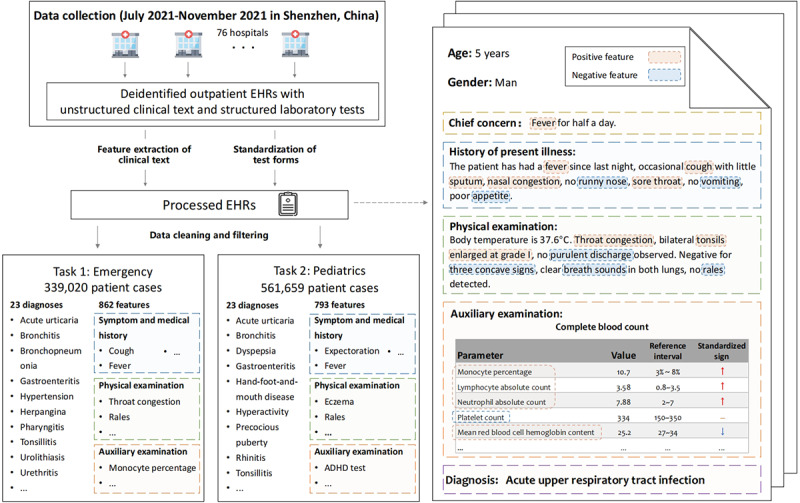
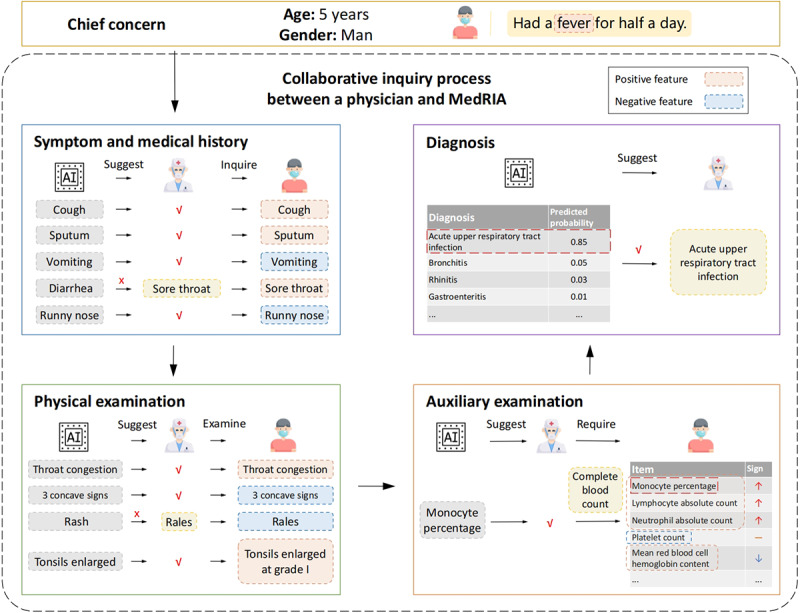
Methods: We compiled multicenter, deidentified outpatient electronic health records from 76 hospitals in Shenzhen, China, spanning the period from July to November 2021. These records consisted of both unstructured textual information and structured laboratory test results. We first performed feature extraction and standardization using natural language processing techniques and then used a reinforcement learning actor-critic framework to explore the rational and effective inquiry logic. To align the inquiry process with actual clinical practice, we segmented the inquiry into 4 stages: inquiring about symptoms and medical history, conducting physical examinations, requesting auxiliary examinations, and terminating the inquiry with a diagnosis. External validation was conducted to validate the inquiry logic of the AI model.
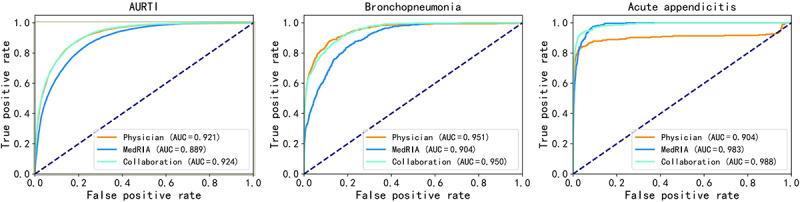
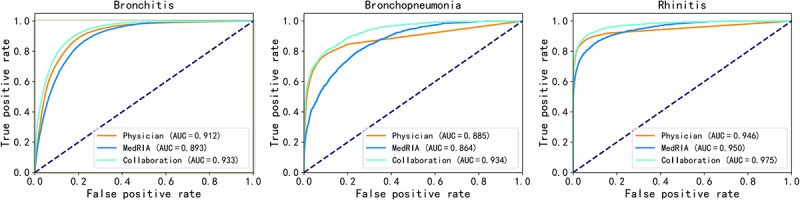
Results: This study focused on 2 retrospective inquiry-and-diagnosis tasks in the emergency and pediatrics departments. The emergency departments provided records of 339,020 consultations including mainly children (median age 5.2, IQR 2.6-26.1 years) with various types of upper respiratory tract infections (250,638/339,020, 73.93%). The pediatrics department provided records of 561,659 consultations, mainly of children (median age 3.8, IQR 2.0-5.7 years) with various types of upper respiratory tract infections (498,408/561,659, 88.73%). When conducting its own inquiries in both scenarios, the AI model demonstrated high diagnostic performance, with areas under the receiver operating characteristic curve of 0.955 (95% CI 0.953-0.956) and 0.943 (95% CI 0.941-0.944), respectively. When the AI model was used in a simulated collaboration with physicians, it notably reduced the average number of physicians' inquiries to 46% (6.037/13.26; 95% CI 6.009-6.064) and 43% (6.245/14.364; 95% CI 6.225-6.269) while achieving areas under the receiver operating characteristic curve of 0.972 (95% CI 0.970-0.973) and 0.968 (95% CI 0.967-0.969) in the scenarios. External validation revealed a normalized Kendall τ distance of 0.323 (95% CI 0.301-0.346), indicating the inquiry consistency of the AI model with physicians.
Conclusions: This retrospective analysis of predominantly respiratory pediatric presentations in emergency and pediatrics departments demonstrated that an AI-driven diagnostic assistant had high diagnostic performance both in stand-alone use and in simulated collaboration with clinicians. Its investigation process was found to be consistent with the clinicians' medical investigation logic. These findings highlight the diagnostic assistant's promise in assisting the decision-making processes of health care professionals.
Keywords: artificial intelligence; electronic health record; inquiry and diagnosis; natural language processing; reinforcement learning.
©Xuan Zou, Weijie He, Yu Huang, Yi Ouyang, Zhen Zhang, Yu Wu, Yongsheng Wu, Lili Feng, Sheng Wu, Mengqi Yang, Xuyan Chen, Yefeng Zheng, Rui Jiang, Ting Chen. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 23.08.2024.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures


Similar articles
-
Pre-Consultation System Based on the Artificial Intelligence Has a Better Diagnostic Performance Than the Physicians in the Outpatient Department of Pediatrics.Front Med (Lausanne). 2021 Nov 8;8:695185. doi: 10.3389/fmed.2021.695185. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34820391 Free PMC article.
-
An Innovative Artificial Intelligence-Based App for the Diagnosis of Gestational Diabetes Mellitus (GDM-AI): Development Study.J Med Internet Res. 2020 Sep 15;22(9):e21573. doi: 10.2196/21573. J Med Internet Res. 2020. PMID: 32930674 Free PMC article.
-
How Clinicians Perceive Artificial Intelligence-Assisted Technologies in Diagnostic Decision Making: Mixed Methods Approach.J Med Internet Res. 2021 Dec 16;23(12):e33540. doi: 10.2196/33540. J Med Internet Res. 2021. PMID: 34924356 Free PMC article.
-
Independent External Validation of Artificial Intelligence Algorithms for Automated Interpretation of Screening Mammography: A Systematic Review.J Am Coll Radiol. 2022 Feb;19(2 Pt A):259-273. doi: 10.1016/j.jacr.2021.11.008. Epub 2022 Jan 20. J Am Coll Radiol. 2022. PMID: 35065909 Free PMC article.
-
Artificial Intelligence Versus Clinicians in Disease Diagnosis: Systematic Review.JMIR Med Inform. 2019 Aug 16;7(3):e10010. doi: 10.2196/10010. JMIR Med Inform. 2019. PMID: 31420959 Free PMC article. Review.
Cited by
-
Large language models for disease diagnosis: a scoping review.NPJ Artif Intell. 2025;1(1):9. doi: 10.1038/s44387-025-00011-z. Epub 2025 Jun 9. NPJ Artif Intell. 2025. PMID: 40607112 Free PMC article. Review.
-
Assessing the Impact on Electronic Health Record Burden After Five Years of Physician Engagement in a Canadian Mental Health Organization: Mixed-Methods Study.JMIR Hum Factors. 2025 May 9;12:e65656. doi: 10.2196/65656. JMIR Hum Factors. 2025. PMID: 40344205 Free PMC article.
References
-
- Musen MA, Middleton B, Greenes RA. Clinical decision-support systems. In: Shortliffe EH, Cimino JJ, editors. Biomedical Informatics: Computer Applications in Health Care and Biomedicine. Cham, Switzerland: Springer; 2021. pp. 795–840.
-
- Sutton RT, Pincock D, Baumgart DC, Sadowski DC, Fedorak RN, Kroeker KI. An overview of clinical decision support systems: benefits, risks, and strategies for success. NPJ Digit Med. 2020;3:17. doi: 10.1038/s41746-020-0221-y. http://europepmc.org/abstract/MED/32047862 221 - DOI - PMC - PubMed
-
- Shickel B, Tighe PJ, Bihorac A, Rashidi P. Deep EHR: a survey of recent advances in deep learning techniques for electronic health record (EHR) analysis. IEEE J Biomed Health Inform. 2018 Sep;22(5):1589–604. doi: 10.1109/JBHI.2017.2767063. https://europepmc.org/abstract/MED/29989977 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
