

Next-generation lung cancer pathology: Development and validation of diagnostic and prognostic algorithms
- PMID: 39178857
- PMCID: PMC11524894
- DOI: 10.1016/j.xcrm.2024.101697
Next-generation lung cancer pathology: Development and validation of diagnostic and prognostic algorithms
Abstract
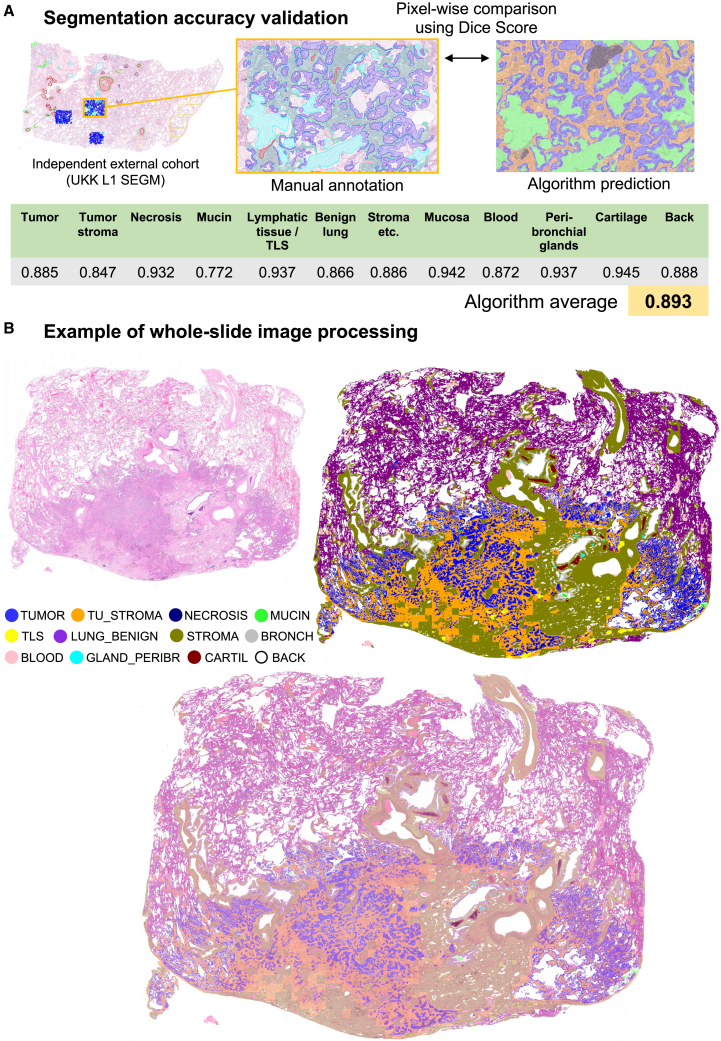
Non-small cell lung cancer (NSCLC) is one of the most common malignant tumors. In this study, we develop a clinically useful computational pathology platform for NSCLC that can be a foundation for multiple downstream applications and provide immediate value for patient care optimization and individualization. We train the primary multi-class tissue segmentation algorithm on a substantial, high-quality, manually annotated dataset of whole-slide images with lung adenocarcinoma and squamous cell carcinomas. We investigate two downstream applications. NSCLC subtyping algorithm is trained and validated using a large, multi-institutional (n = 6), multi-scanner (n = 5), international cohort of NSCLC cases (slides/patients 4,097/1,527). Moreover, we develop four AI-derived, fully explainable, quantitative, prognostic parameters (based on tertiary lymphoid structure and necrosis assessment) and validate them for different clinical endpoints. The computational platform enables the high-precision, quantitative analysis of H&E-stained slides. The developed prognostic parameters facilitate robust and independent risk stratification of patients with NSCLC.
Keywords: AI; NSCLC; algorithm; lung cancer; prognosis; subtyping.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures







References
-
- Siegel R.L., Miller K.D., Wagle N.S., Jemal A. Cancer statistics, 2023. CA. Cancer J. Clin. 2023;73:17–48. - PubMed
-
- Zhang Y., Vaccarella S., Morgan E., Li M., Etxeberria J., Chokunonga E., Manraj S.S., Kamate B., Omonisi A., Bray F. Global variations in lung cancer incidence by histological subtype in 2020: a population-based study. Lancet Oncol. 2023;24:1206–1218. - PubMed
-
- El Nahhas O.S.M., Loeffler C.M.L., Carrero Z.I., van Treeck M., Kolbinger F.R., Hewitt K.J., Muti H.S., Graziani M., Zeng Q., Calderaro J., et al. Regression-based Deep-Learning predicts molecular biomarkers from pathology slides. Nat. Commun. 2024;15 doi: 10.1038/S41467-024-45589-1. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
