

Comparative analysis among therapeutic modalities in ruptured hepatocellular carcinoma and identification of imaging predictors for survival
- PMID: 39183268
- PMCID: PMC11346290
- DOI: 10.1186/s12885-024-12829-y
Comparative analysis among therapeutic modalities in ruptured hepatocellular carcinoma and identification of imaging predictors for survival
Abstract
Background: Spontaneous rupture of hepatocellular carcinoma (rHCC) poses a life-threatening complication with a mortality rate of 25-75%. Treatment aims at achieving hemostasis and includes options such as trans-arterial embolization, perihepatic packing, and hepatic resection. The optimal treatment remains a subject of debate. Our retrospective review evaluates these treatments and investigates imaging's role in prognosis for rHCC patients.
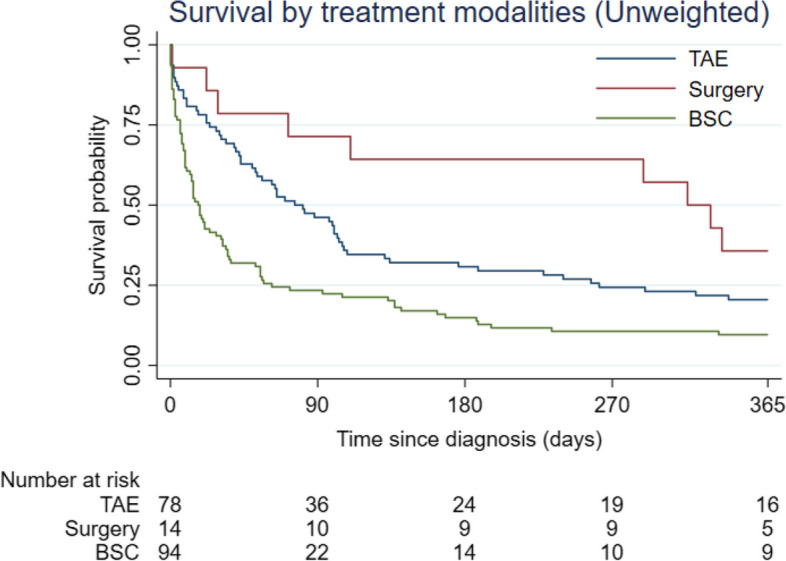
Purpose: We aimed to compare survival outcomes among rHCC patients who received transarterial embolization (TAE), surgery (perihepatic packing, hepatectomy), or best supportive care (BSC), while also identifying predictive imaging factors in these patients.
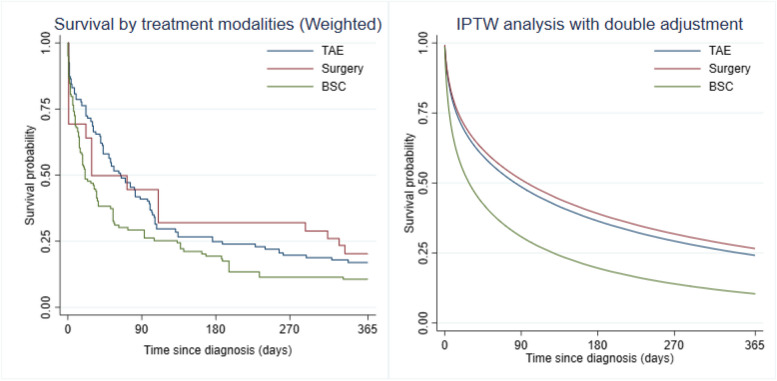
Materials and methods: All patients diagnosed with rHCC and admitted to Maharaj Nakorn Chiangmai Hospital between January 2012 and December 2021 were included. We reviewed clinical features, imaging results, treatment modalities, and outcomes. In order to balance pretreatment confounders, inverse probability treatment weighting (IPTW) was employed. Flexible parametric survival regression was utilized to compare survival outcomes and identify imaging factors predicting the survival of rHCC patients. Hazard ratios (HR) and the difference in restricted mean survival time (RMST) were reported.
Result: Among the 186 rHCC patients included, we observed 90-day and 1-year mortality rates of 64% and 84%, respectively. Both the TAE and surgery groups exhibited significantly lower 1-year mortality rates compared to BSC. The HR were 0.56 (95% CI 0.33-0.96) for TAE and 0.52 (95% CI 0.28-0.95) for surgery compared to BSC. Both the TAE and surgery also significantly extended the 1-yeaar life expectancy post-initial treatment when compared to BSC, with an RMST difference of + 55.40 days (95% CI 30.18-80.63) for TAE vs. BSC and + 68.43 days (95% CI 38.77-98.09) for surgery vs. BSC. The presence of active contrast extravasation and bleeding in both lobes were independent prognostic factors for 1-year survival.
Conclusions: TAE and surgical treatments provide comparable survival benefits for rHCC patients, extending survival time by approximately 2 months compared to best supportive care. We strongly recommend active management for all rHCC patients whenever possible.
Keywords: Hepatectomy; Perihepatic packing; Rupture hepatocellular carcinoma; Transarterial embolization.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





References
-
- Kirikoshi H, Saito S, Yoneda M, Fujita K, Mawatari H, Uchiyama T, Higurashi T, Imajo K, Sakaguchi T, Atsukawa K, et al. Outcomes and factors influencing survival in cirrhotic cases with spontaneous rupture of hepatocellular carcinoma: a multicenter study. BMC Gastroenterol. 2009;9(1):29. 10.1186/1471-230X-9-29 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
