

Probable idiopathic hypereosinophilic syndrome: A case report of severe multi-organ eosinophilic involvement in a young male presenting with heart failure
- PMID: 39185068
- PMCID: PMC11342427
- DOI: 10.1177/2050313X241272551
Probable idiopathic hypereosinophilic syndrome: A case report of severe multi-organ eosinophilic involvement in a young male presenting with heart failure
Abstract
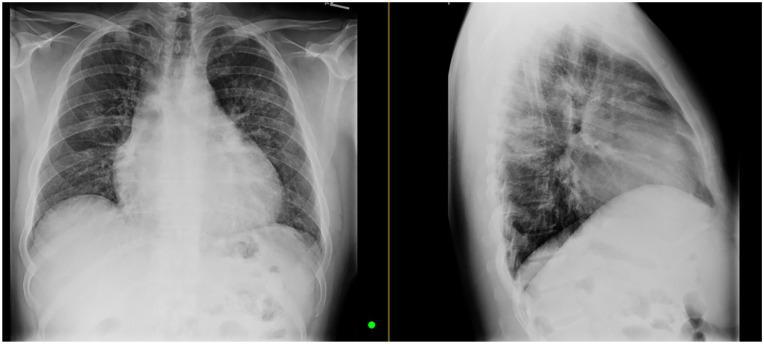
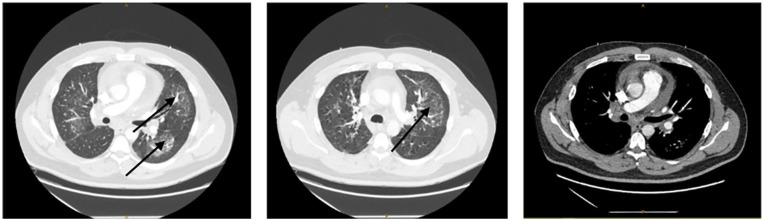
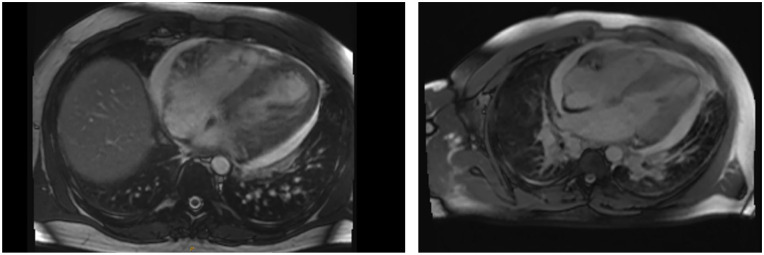
Hypereosinophilic syndrome (HES) is a disorder characterized by elevated levels of eosinophils, which may be associated with multi-organ involvement depending on severity. The recent diagnostic criteria for idiopathic HES require an elevated absolute eosinophil count (AEC) above 1500 cells/mcL with evidence of tissue damage. We present a case of a 37-year-old male firefighter with a purported history of eosinophilic bronchitis who was referred to the hospital with syncopal episodes and a persistent productive cough. The patient showed an AEC of 4500 cells/mcL on admission associated with high inflammatory markers. Cardiac imaging demonstrated acute myocarditis with heart failure and a reduced ejection fraction. Chest imaging was initially suggestive of community-acquired pneumonia. Workup was negative for a malignant etiology; infectious causes similarly were excluded. After a multidisciplinary evaluation, a diagnosis of idiopathic HES was made and steroids were instituted with rapid resolution of symptoms. Our case illustrates the importance of considering hypereosinophilia as a precipitating factor for acute heart failure in an otherwise healthy adult. An expeditious diagnosis can lead to early initiation of steroids to avoid progression toward multi-organ failure.
Keywords: Acute systolic heart failure; hypereosinophilia; idiopathic; idiopathic hypereosinophilic syndrome; myocarditis; pericardial effusion; reduce risk of death; urgent treatment.
© The Author(s) 2024.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Gotlib J. World Health Organization-defined eosinophilic disorders: 2017 update on diagnosis, risk stratification, and management. Am J Hematol 2017; 92(11): 1243–1259. - PubMed
-
- RegiSCAR score for drug reaction with eosinophilia and systemic symptoms (DRESS) [Internet]. MDCalc, https://www.mdcalc.com/calc/10084/regiscar-score-drug-reaction-eosinophi... (2009, accessed 11 July 2024).
Publication types
LinkOut - more resources
Full Text Sources
