

This is a preprint.
Automated Craniofacial Biometry with 3D T2w Fetal MRI
- PMID: 39185514
- PMCID: PMC11343257
- DOI: 10.1101/2024.08.13.24311408
Automated Craniofacial Biometry with 3D T2w Fetal MRI
Update in
-
Automated craniofacial biometry with 3D T2w fetal MRI.PLOS Digit Health. 2024 Dec 30;3(12):e0000663. doi: 10.1371/journal.pdig.0000663. eCollection 2024 Dec. PLOS Digit Health. 2024. PMID: 39774200 Free PMC article.
Abstract
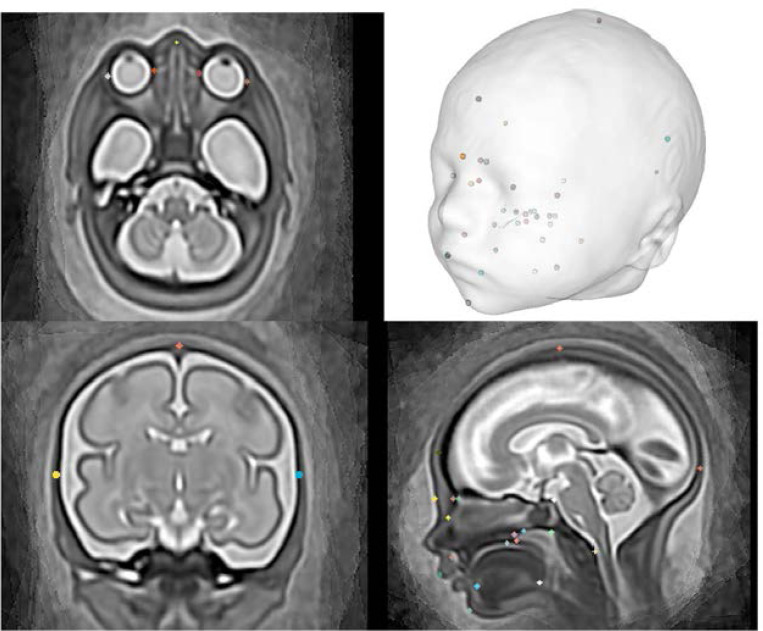
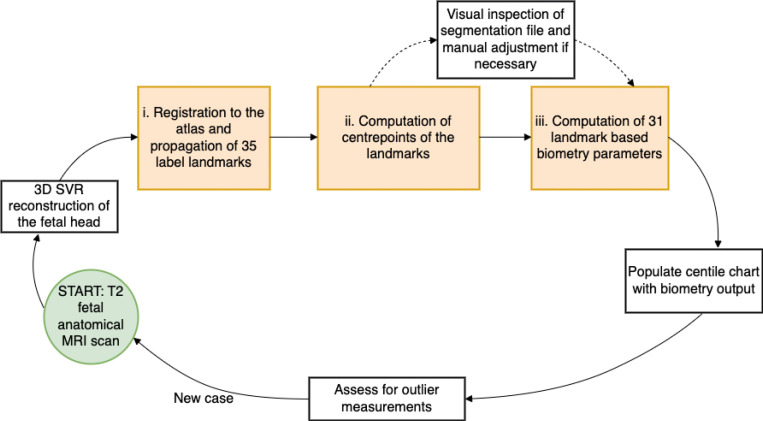
Objectives: Evaluating craniofacial phenotype-genotype correlations prenatally is increasingly important; however, it is subjective and challenging with 3D ultrasound. We developed an automated landmark propagation pipeline using 3D motion-corrected, slice-to-volume reconstructed (SVR) fetal MRI for craniofacial measurements.
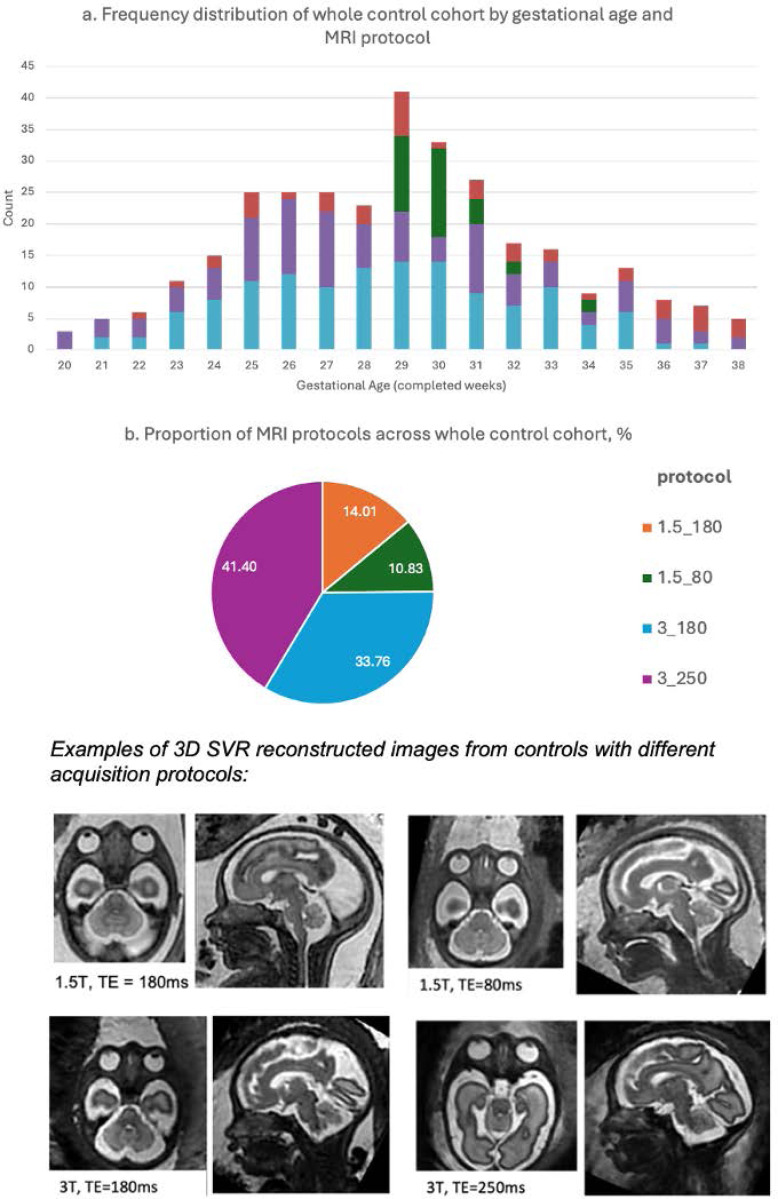
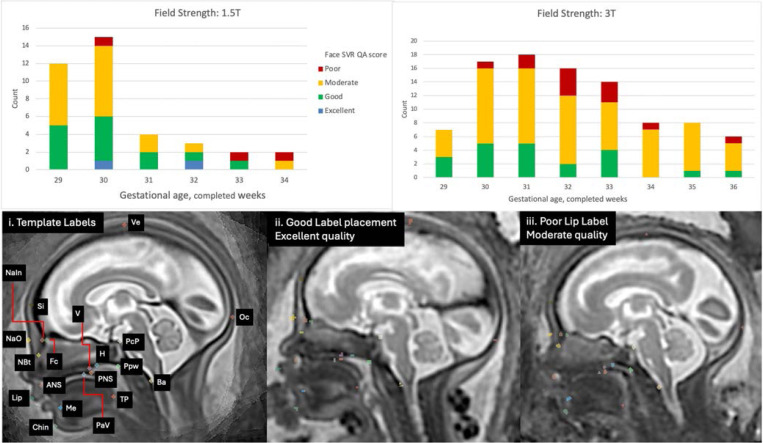
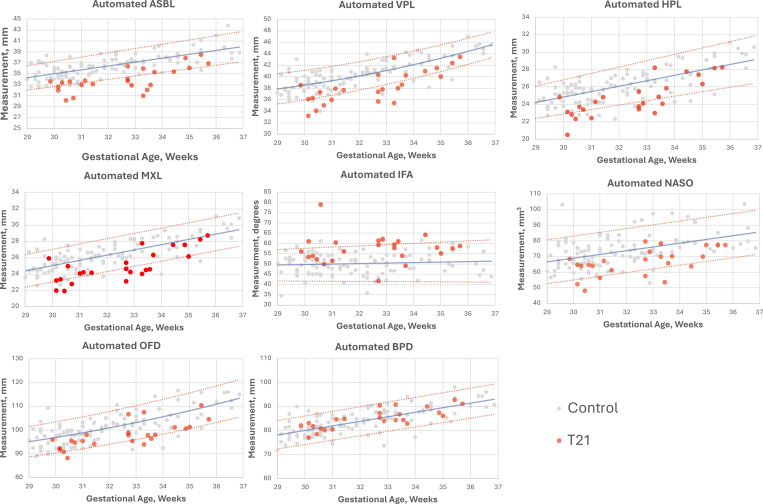
Methods: A literature review and expert consensus identified 31 craniofacial biometrics for fetal MRI. An MRI atlas with defined anatomical landmarks served as a template for subject registration, auto-labelling, and biometric calculation. We assessed 108 healthy controls and 24 fetuses with Down syndrome (T21) in the third trimester (29-36 weeks gestational age, GA) to identify meaningful biometrics in T21. Reliability and reproducibility were evaluated in 10 random datasets by four observers.
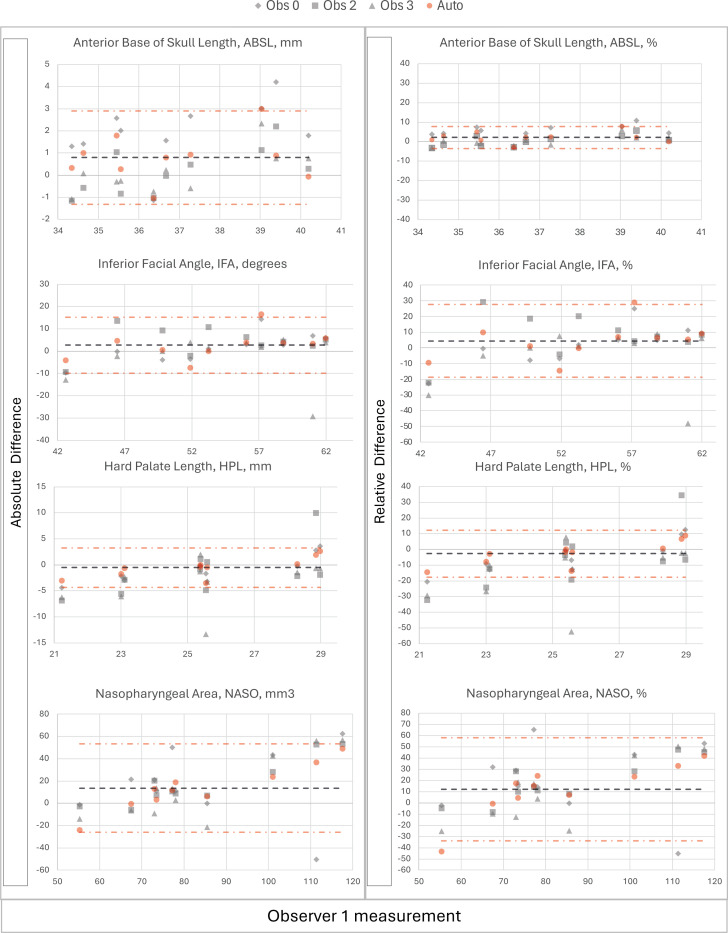
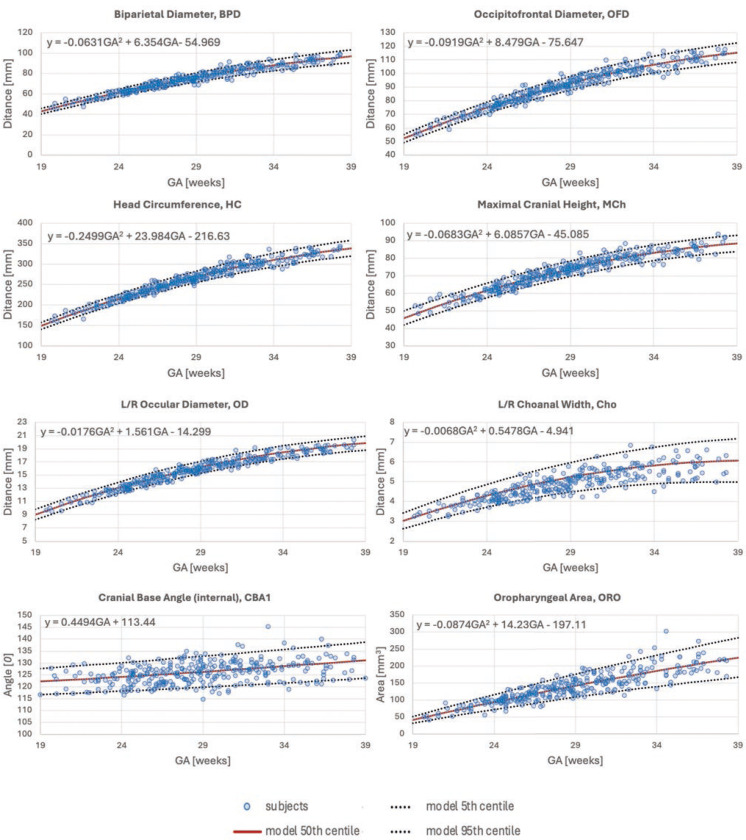
Results: Automated labels were produced for all 132 subjects with a 0.03% placement error rate. Seven measurements, including anterior base of skull length and maxillary length, showed significant differences with large effect sizes between T21 and control groups (ANOVA, p<0.001). Manual measurements took 25-35 minutes per case, while automated extraction took approximately 5 minutes. Bland-Altman plots showed agreement within manual observer ranges except for mandibular width, which had higher variability. Extended GA growth charts (19-39 weeks), based on 280 control fetuses, were produced for future research.
Conclusion: This is the first automated atlas-based protocol using 3D SVR MRI for fetal craniofacial biometrics, accurately revealing morphological craniofacial differences in a T21 cohort. Future work should focus on improving measurement reliability, larger clinical cohorts, and technical advancements, to enhance prenatal care and phenotypic characterisation.
Conflict of interest statement
Additional information Competing interests The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Automated craniofacial biometry with 3D T2w fetal MRI.PLOS Digit Health. 2024 Dec 30;3(12):e0000663. doi: 10.1371/journal.pdig.0000663. eCollection 2024 Dec. PLOS Digit Health. 2024. PMID: 39774200 Free PMC article.
-
Automated 3D reconstruction of the fetal thorax in the standard atlas space from motion-corrupted MRI stacks for 21-36 weeks GA range.Med Image Anal. 2022 Aug;80:102484. doi: 10.1016/j.media.2022.102484. Epub 2022 May 25. Med Image Anal. 2022. PMID: 35649314 Free PMC article.
-
BOUNTI: Brain vOlumetry and aUtomated parcellatioN for 3D feTal MRI.bioRxiv [Preprint]. 2023 Apr 27:2023.04.18.537347. doi: 10.1101/2023.04.18.537347. bioRxiv. 2023. PMID: 37131820 Free PMC article. Preprint.
-
3D T2w fetal body MRI: automated organ volumetry, growth charts and population-averaged atlas.medRxiv [Preprint]. 2023 Sep 18:2023.05.31.23290751. doi: 10.1101/2023.05.31.23290751. medRxiv. 2023. Update in: Sci Rep. 2024 Mar 19;14(1):6637. doi: 10.1038/s41598-024-57087-x. PMID: 37398121 Free PMC article. Updated. Preprint.
-
Biometric and morphological features on magnetic resonance imaging of fetal bladder in lower urinary tract obstruction: new perspectives for fetal cystoscopy.Ultrasound Obstet Gynecol. 2020 Jul;56(1):86-95. doi: 10.1002/uog.20297. Ultrasound Obstet Gynecol. 2020. PMID: 31006924
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources