

This is a preprint.
Prediction of Postoperative Delirium in Older Adults from Preoperative Cognition and Occipital Alpha Power from Resting-State Electroencephalogram
- PMID: 39185530
- PMCID: PMC11343253
- DOI: 10.1101/2024.08.15.24312053
Prediction of Postoperative Delirium in Older Adults from Preoperative Cognition and Occipital Alpha Power from Resting-State Electroencephalogram
Update in
-
Prediction of postoperative delirium in older adults from preoperative cognition and occipital alpha power from resting-state electroencephalogram.Age Ageing. 2025 Oct 30;54(11):afaf330. doi: 10.1093/ageing/afaf330. Age Ageing. 2025. PMID: 41222553
Abstract
Background: Postoperative delirium is the most common complication following surgery among older adults, and has been consistently associated with increased mortality and morbidity, cognitive decline, and loss of independence, as well as markedly increased health-care costs. Electroencephalography (EEG) spectral slowing has frequently been observed during episodes of delirium, whereas intraoperative frontal alpha power is associated with postoperative delirium. We sought to identify preoperative predictors that could identify individuals at high risk for postoperative delirium, which could guide clinical decision-making and enable targeted interventions to potentially decrease delirium incidence and postoperative delirium-related complications.
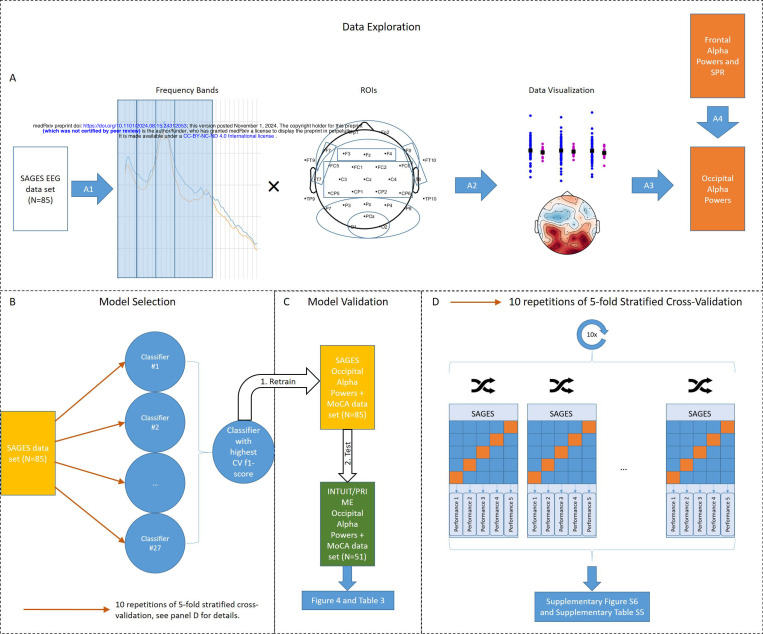
Methods: In this prospective observational study, we used machine learning to evaluate whether baseline (preoperative) cognitive function and resting-state EEG could be used to identify patients at risk for postoperative delirium. Preoperative resting-state EEGs and the Montreal Cognitive Assessment were collected from 85 patients (age = 73 ± 6.4 years, 12 cases of delirium) undergoing elective surgery. The model with the highest f1-score was subsequently validated in an independent, prospective cohort of 51 older adults (age = 68 ± 5.2 years, 6 cases of delirium) undergoing elective surgery.
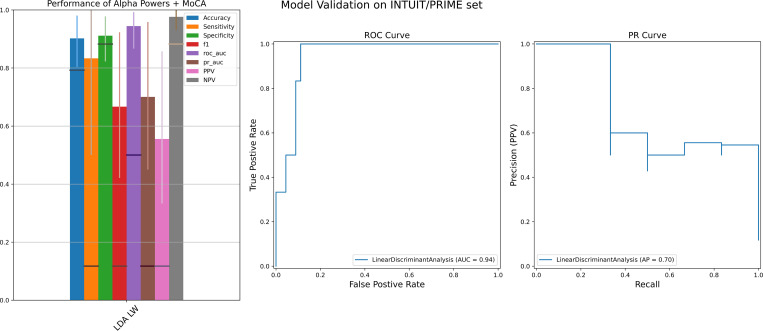
Results: Occipital alpha powers have higher f1-score than frontal alpha powers and EEG spectral slowing in the training cohort. Occipital alpha powers were able to predict postoperative delirium with AUC, specificity and accuracy all >90%, and sensitivity >80%, in the validation cohort. Notably, models incorporating transformed alpha powers and cognitive scores outperformed models incorporating occipital alpha powers alone or cognitive scores alone.
Conclusions: While requiring prospective validation in larger cohorts, these results suggest that strong prediction of postoperative delirium may be feasible in clinical settings using simple and widely available clinical tools. Additionally, our results suggested that the thalamocortical circuit exhibits different EEG patterns under different stressors, with occipital alpha powers potentially reflecting baseline vulnerabilities.
Conflict of interest statement
Dr. E. Santarnecchi serves on the scientific advisory boards for BottNeuro, which has no overlap with present work; and is listed as an inventor on several issued and pending patents on brain stimulation solutions to diagnose or treat neurodegenerative disorders and brain tumors. Dr. A. Pascual-Leone is a co-founder of Linus Health and TI Solutions AG which have no overlap with present work. He serves on the scientific advisory boards for the ACE Foundation and the IT’IS Foundation, Neuroelectrics, TetraNeuron, Skin2Neuron, MedRhythms, and Magstim Inc; and is listed as an inventor on several issued and pending patents on the real-time integration of noninvasive brain stimulation with electroencephalography and magnetic resonance imaging, applications of noninvasive brain stimulation in various neurological disorders, as well as digital biomarkers of cognition and digital assessments for early diagnosis of dementia. Dr. M Berger has received private legal consulting fees related to perioperative neurocognitive disorders. None of the other authors report any conflicts of interest. All the other co-authors fully disclose they have no financial interests, activities, relationships and affiliations. The other co-authors also declare they have no potential conflicts in the three years prior to submission of this manuscript.
Figures


References
-
- American Psychiatric Association, American Psychiatric Association: Diagnostic and statistical manual of mental disorders: DSM-5, 5th ed. Washington, D.C, American Psychiatric Association, 2013
-
- Yan E, Veitch M, Saripella A, et al. : Association between postoperative delirium and adverse outcomes in older surgical patients: A systematic review and meta-analysis. J Clin Anesth 2023; 90:111221. - PubMed
-
- Dolan MM, Hawkes WG, Zimmerman SI, et al. : Delirium on hospital admission in aged hip fracture patients: prediction of mortality and 2-year functional outcomes. J Gerontol A Biol Sci Med Sci 2000; 55:M527–534 - PubMed
-
- Ely EW, Shintani A, Truman B, et al. : Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA 2004; 291:1753–62 - PubMed
-
- Ouimet S, Kavanagh BP, Gottfried SB, Skrobik Y: Incidence, risk factors and consequences of ICU delirium. Intensive Care Med 2007; 33:66–73 - PubMed
Publication types
Grants and funding
- R01 AG051658/AG/NIA NIH HHS/United States
- K76 AG057022/AG/NIA NIH HHS/United States
- K24 AG035075/AG/NIA NIH HHS/United States
- R01 MH115949/MH/NIMH NIH HHS/United States
- R01 AG060987/AG/NIA NIH HHS/United States
- R24 AG054259/AG/NIA NIH HHS/United States
- R01 AG073598/AG/NIA NIH HHS/United States
- R33 AG071744/AG/NIA NIH HHS/United States
- R03 AG072233/AG/NIA NIH HHS/United States
- R01 EB032820/EB/NIBIB NIH HHS/United States
- P01 AG031720/AG/NIA NIH HHS/United States
- R01 AG059089/AG/NIA NIH HHS/United States
- P30 AG072958/AG/NIA NIH HHS/United States
- P30 AG028716/AG/NIA NIH HHS/United States
- R01 AG076708/AG/NIA NIH HHS/United States
- UH2 AG056925/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources